
Editor’s note: This two-part roundtable features critiques of contemporary visual culture as seen through a medical humanist lens. Part I drew on research in sociology to interpret pharmaceutical advertising. In Part II, below, Leah Rosen and Lilli Schussler tackle questions of the reproduction and extension of human life: Rosen in the context of 1930s popular writing on eugenics, and Schussler on how contemporary advertising mobilizes biopower to sell cancer treatments.
The American Legacy of “Uterus Collectors”: A Condemnation of Physical Culture and Eugenics
Leah Rosen //
“What is he? Is he the uterus collector?”
–Woman detained in Irwin County Detention Center
While this quote evokes an image from nightmares and horror films alike—of a man collecting the uteruses of his female victims—it could instead describe the actions of Dr. Mahendra Amin, a physician employed at an ICE detention center in South Georgia, who is accused of performing mass (perhaps forced) hysterectomies on female detainees. These claims were brought to the attention of the American public in September 2020 by Dawn Wooten, a nurse at the Irwin County Detention Center who described the aforementioned abuses, along with failure to comply with COVID-19 guidelines, as evidence of the ICE facility’s general neglect for the detainees. Although Wooten’s claims have yet to be confirmed by investigators, they warrant serious concern over the well-being of detained people. In addition, these claims—namely, of mass hysterectomies and the abuse of immigrants—are sadly consistent with the American legacy of eugenics and social injustice. These forced hysterectomies fit neatly into a grim historical narrative of medical racism and violence in the United States which has rendered some bodies privileged and other bodies available for experimentation and manipulation.
In the late 19th century, the British anthropologist Francis Galton coined the term “eugenics” to mean “well-born.” Galton ascribed to what some now refer to as “positive eugenics,” meaning his ideas were directed toward improving the human population by encouraging “healthy” individuals to procreate. However, as Galton’s ideas spread to the United States and intersected with preexisting sociocultural biases among Americans, a brand of “negative eugenics” developed: one which put forth the belief that certain individuals should not procreate, for the benefit of society overall. To be sure, both “positive” and “negative” eugenics practices are problematic and concerning, but they function in different ways.

The Physical Culture magazine cover from the 1930s (above) mobilizes both forms of eugenics and thus allows us to differentiate between the two. The magazine cover draws the observer’s eye to the woman in the center: a white-presenting, slim, and fashionable woman spending a leisurely day at the beach. To the right of this woman are titles of stories that fit neatly within the boundaries of traditional American family-planning tropes. One features marital advice, another alludes to the importance of finding a “good” man, and the third takes readers on a tour of the organ most frequently associated with love. Together, the woman’s image and the stories referenced on the right side of the magazine cover communicate a positive eugenic statement: love, marriage, and eventually procreation are expected from women who look like this. However, the bottom left corner of the cover references an article written by Albert Edward Wiggam—a renowned eugenicist, whose writings were praised by Hitler—titled “Shall We Breed or Sterilize Defectives?”. This proposed question, and its assumption that readers of the magazine hold decisional authority over the matter, is a profoundly disturbing example of negative eugenics. By asking “Shall we?”, Wiggam casts his audience—presumably individuals who resemble the racial, socioeconomic, cultural, or educational profile of the woman depicted on the cover—as having the power to determine the reproductive fate of women considered to be somehow lesser, somehow “defective.”
So who were these “defective” women? They were the country’s most vulnerable persons. They were individuals who were cast as “mentally deficient,” who suffered from mental illness, who belonged to minority ethnic or racial groups, or who were dependent on financial welfare assistance—as evidenced in the lives of Carrie Buck , Lucille Schreiber, Elaine Riddick, and Nial Ramirez. And though I list these classifications in the past tense, I hope to demonstrate through the recently-alleged sterilizations of women at the Irwin Detention Center that the American Eugenics Movement is not over. Indeed, the actions of Dr. Amin suggest that there is still bias when it comes to the question of who should reproduce and who should not, and our medical system can serve as the vehicle through which such harmful biases are reproduced.
While Dr. Amin’s abusive actions may be rare among medical professionals, the modern era of medicine possesses other means of controlling female reproduction—means that indeed resemble attempts at social control, in the Foucauldian sense of reducing “deviance” among the body politic. Just as women from marginalized groups are disproportionately represented among the victims of forced sterilization, the patterns of contraception, abortion, and maternal health in the United States similarly show evidence of ableism, racism, and classism. Considering contraception specifically, disability advocates have illuminated how the forced sterilization of individuals with disabilities has merely been eclipsed by recommending early and long-term birth control for them; since the advent of the pill, critical race scholars have linked it to white supremacy efforts; and we cannot forget that low-income Puerto Rican women were used as the initial “guinea pigs” for testing contraception techniques. Further, while the topic of abortion receives significant attention in politics and the media, few are discussing the fact that persons with disabilities are exhaustively used as a political pawn in the conversation, or that anti-abortion beliefs are historically rooted in racial issues, or that a majority of women who receive abortions are from low socio-economic backgrounds. And finally, when analyzing the access to and quality of maternal healthcare, women with either a mental illness or disability, from a minority ethnic or racial group, or with fewer socioeconomic resources are more likely to face barriers to perinatal care than their more privileged counterparts.
Yet modern eugenics is not only taking place in clinical spaces. Eugenics was, in fact, a major election issue this year: insofar as the presidential candidates were divided on their opinions about whether racism is a serious national concern, one was promoting eugenics while the other was not. Eugenics is the action of deliberately shaping a body politic, so by upholding white supremacy—and thus spreading beliefs that the whiteness of the United States population needs to be actively preserved—Donald Trump has propagated positive eugenics. But Trump’s eugenic actions do not stop there. He has also promoted negative eugenics—and, frankly, genocide—by failing to intervene in the senseless murders of black Americans, such as George Floyd and Breonna Taylor. Furthermore, Trump’s insistence on holding public gatherings during a widespread pandemic—knowing that COVID-19 is indeed infectious and causing particular harm to black and Latinx communities—resulted in deaths that were otherwise avoidable. These actions demonstrate a prolific and intentional effort to protect American whiteness at the expense of other lives. Does it sound like eugenics yet?
Perhaps most concerningly, Trump’s eugenic agendas are neither discreet nor covert. He has referred explicitly to his goals of preserving the white American majority, as well as his beliefs in social Darwinism. For instance, while speaking on September 18th in Bemidji, Minnesota—a predominantly white city in an overwhelmingly white state, which has recently become a destination for Somalian refugees—Trump exclaimed to the sea of white, mask-less faces, “You have good genes, you know that, right? You have good genes. A lot of it is about genes, isn’t it, don’t you believe? The racehorse theory? … You have good genes in Minnesota.” The “racehorse theory” suggests that there are superior members of the human race who have so-called “good genes.” Just as racehorses are bred to possess desirable traits, individuals who ascribe to the “racehorse theory” believe that the same rules of control can and should be applied to the human population. This logic, especially when in the context of white Minnesotans and Somalian refugees, is incredibly troubling—and eugenic.
Before we can begin to address our country’s issues, we need to call them what they are. The examples I have outlined above—ranging from forced sterilizations to unequal access to medical care to systemic and political oppression—are each distinct and real occurrences of eugenics in the modern world. We need to direct our attention to the groups of individuals who are affected, be more compassionate witnesses to their experiences, recognize the extent to which their bodies and rights have been sequestered by social forces of control, and advocate for their freedom. Change seldom comes through silence, so I urge physicians and other care providers, as well as political representatives and leaders, to speak out against reproductive injustice—not on behalf of women, but in concert with them. The renowned Audre Lorde writes, “My silences had not protected me, your silence will not protect you.” Silence only protects those who are already privileged and empowered. Silence protected Dr. Amin, allowing him to continue to perform hysterectomies while the immigrant women continued to suffer. Then Dawn Wooten spoke out, passing along the concerns that were voiced by the female detainees. So some might think that the solution resides in Wooten’s speaking out—as if, finally, someone said something. But Wooten was merely quoting the detainees, who may have indeed been voicing their concerns the entire time.
Instead, I think: finally someone was listening.
Author bio: Leah Rosen is a student in the Narrative Medicine Master of Science program at Columbia University. She graduated from Duke University in 2019, where she created an interdisciplinary major titled “Illness and Identity.” Her academic interests include the medical humanities, epistemology, narrative therapy, and social justice. Her work has recently appeared in Scientific American and Please See Me. Contact Leah at leah.rosen44@gmail.com.
Opdivo: Shining a Light on Biopower
Health interventions or technologies whose primary benefit is the extension of the lifespan call into question the political nature of death in modernity: when should we die? When do we want to die? And how do the predominant narratives associated with life and death promote the interests of the modern biopolitical state in managing life? Michel Foucault defines biopower as power that is “focused on the species body, the body imbued with the mechanics of life and serving as the basis for the biological processes.” While his formation of disciplinary power is concerned with the individuals who constitute institutions, biopower operates on the level of the population, or species-body, and is concerned with rates, especially those pertaining to birth and death (History 141). Because the aim of biopower is the management of life, death becomes “scandal”: per Foucault, death is the moment the subject escapes power and, as such, death is a medical problem to be mastered through the creation of knowledge (Society 248). Whereas the motto of classical sovereignty (until the end of the 17th century and as exemplified by the monarchy) might be characterized as “take life or let live,” the motto of the modern biopower state is “make live or let die” (History 136).
In the following analysis, I apply Foucault’s concepts of biopower and the subject to a video advertisement for Opdivo (nivolumab), a chemotherapeutic drug for individuals with metastatic small cell lung cancer. Crucial to my analysis is the sole statistic in the ad: “In a clinical trial of non-squamous patients, half of those on OPDIVO were alive at 12.2 months versus 9.4 months for chemotherapy (docetaxel).” Opdivo thus offers patients an average of three additional months of life as compared to the control drug. Although the ad initially seems to be a composite of individual narratives, I argue that the Foucauldian notion of biopower operates throughout the video and is communicated through the use of light. In the video, light, manifest in various forms, surreptitiously hijacks the lives of the patients by posing the drug as a choice between life and death and thereby normalizing the desire to prolong life. The drug thus becomes a locus of biopower: its objective is to administer life and to create subjects who have internalized the desire for this administration.
In the ad, light is used to convey Opdivo’s mortality benefit and to normalize the desire to extend life. All of the core messages and information featured in the advertisement are communicated through luminous projections onto various pedestrian structures: building facades, sidewalks, walls. Each time a projected message about Opdivo appears, patients and their (presumed) family members pause what they are doing to gaze with a sense of wonder and hope, and the orchestra music builds sympathetically.

The projection onto buildings is reminiscent of flashes of light in Judeo-Christian religious visions, such as that of Paul (formerly Saul) the Apostle before his conversion. Saul is blinded by a flash of light from heaven followed by the words of G-d: “Saul, Saul, why do you persecute me?” (New American Standard Bible, Acts 9:4). Now Paul, newly anointed by G-d, begins the second act of his life, and preaches the word of Christ. The projected messages thus evoke religious associations of light with hope, new beginnings, and even a chance of redemption.
In addition to the projected messages, the ad also uses natural lighting to normalize the desire to extend the lifespan. In each of the pedestrian scenes, the sun is setting, and patients are cast in shadow until they are illuminated by the light of Opdivo messages. In one scene, a man and his wife descend an outdoor staircase at sunset. The light captures their attention and causes them to turn around to view the complete line: “OPDIVO significantly increased the chance of living longer versus chemotherapy.” The drug thereby becomes an opportunity for patients who are descending in the arc of life, toward the grave, to turn around and ascend a few steps—or even to ascend completely. The dichotomy between life and death is represented by the contrast between light and darkness: light conveys hope, perseveration, and scientific breakthrough; darkness, in contrast, implicitly represents disease and death, ignorance, and acquiescence to illness.
Discourses, according to Foucault, encompass more than epistemology and semiotics: they dictate “the ‘nature’ of the body, unconscious and conscious mind and emotional life of the subjects they seek to govern” (Weedon 172). In the case of the ad, the question is not how the concept of more life is sold, but rather, how the prolongation of the lifespan assumes the “status of truth” (Yazdannik et al). Most modern forms of discipline do not require the use of force and instead rely on self-policing (Society); accordingly, the people in the ad do not require convincing to choose more life. Though the ad includes two brief scenes that suggest what patients could do with more life (of note, both are generation-bridging, grandparent-grandchild activities), the ad is overall less concerned with the persuasion of its actors and viewers than it is with the normalization of the will to live. While more time to play with grandchildren is certainly a plus, it is light that captures the imagination of the actors and viewers alike and is used to pose the extension of the lifespan as an empirically true and universal desire. Whether interpreted as religious revelation or technological breakthrough, light is empirically captivating and necessary, as patients navigate the twilight of their lives in literal darkness.
The individuals in the ad are subjects of biopower in that they voluntarily stop what they are doing to receive the Opdivo messages, and they receive these messages with what appears to be unquestioning reverence. The possibility of extending the lifespan is not just enticing; it is what the patients were looking for all along, and without which they would remain in darkness.

The only scene that is not at sunset takes place a little later in the day, at dusk. Two women stop walking to examine an Opdivo infographic projected onto a building. They contemplate a luminous, faceless blue figure, which is several stories high and depicted from the waist up. The figure has no discernible organs aside from lungs. The infographic presumably shows an increased number of active T-cells in the lungs due to the drug and, unsurprisingly, bears no other scientific import. The mesmerizing quality of the blue infographic captures the attention of both the subjects and the viewer. The patients are drawn to the light, again evoking a religious revelation and an irresistible quality to the drug. The advertisement implores: how could you not look away? How could you say “no” to more life? The contrast between the massive, illuminated human model and the relatively smaller patients in the darkness suggests that without the drug, patients are not only left in scientific darkness and ignorance—they are also vulnerable and distanced from the divine.
The scene is reminiscent of a print of the frontispiece of the Encyclopédie (1772), originally drawn by Charles-Nicolas Cochin and engraved by Bonaventure-Louis Prévost.
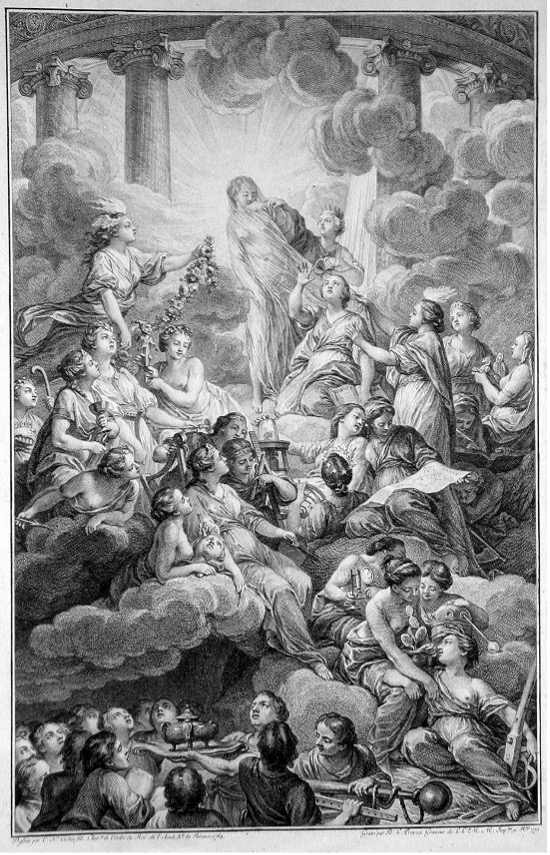
The figure at the center is Truth, bathed in light—the chief symbol of the Enlightenment era. To her right, Reason and Philosophy tear her veil. Truth is clearly associated with divinity: she is closest to the pillars of Mount Olympus. The figures surrounding Truth are closer to the light and are also depicted as holy. They don regal robes, are festooned with flowers and wreathes, and sit or stand atop clouds. In contrast, the figures at the bottom, wear dark, civilian clothing and have dark hair. These figures grasp at straws to find Truth, using offerings and measures—but their attempts are clearly in vain, as they remain in the dark, yearning for light. The actors in the dusk scene of the Opdivo ad are the modern incarnation of the civilians in the drawing: fumbling, desperate, and mortal.
Works Cited
Bonaventure-Louis Prévost (engraver). Frontispiece to the Encyclopédie. Original drawing by Charles-Nicolas Cochin. 1772. The British Museum, https://www.britishmuseum.org/collection/object/P_1873-0510-3612.
Foucault, M. The History of Sexuality: An Introduction Volume 1,Vintage Books, 1976.
Foucault, M., Bertani, M., Fontana, A., Macey, D. Society must be defended: Lectures at the Collège de France, 1975-1976, Picador, 2003.
Gutting, Gary, and Johanna Oksala. “Michel Foucault.” Stanford Encyclopedia of Philosophy, Stanford University, 22 May 2018, plato.stanford.edu/entries/foucault/.
Mohammadi, Sepideh, et al. “Discourse Analysis: A Useful Methodology for Health-Care System Researches.” Journal of Education and Health Promotion, vol. 6, no. 1, 2017, p. 111., doi:10.4103/jehp.jehp_124_15.
New American Standard Bible. Bible Gateway. https://www.biblegateway.com/passage/?search=Acts+9. Accessed 20 Oct. 2020.
“Opdivo Commercial – New Hope – You almost want what they’re curing.” Youtube. Posted by Excelsior10000. 9 Jan. 2017, https://www.youtube.com/watch?v=7VEZBVT_a3M
Weedon, Chris. Feminist Practice & Poststructuralist Theory. Blackwell Pub., 1997.
Yazdannik, Ahmadreza et al. “Discourse Analysis: A Useful Methodology for Health-Care System Researches.” Journal of Education and Health Promotion, vol. 6, no. 1, 2017, p. 111., doi:10.4103/jehp.jehp_124_15.
Author bio: Lilli Schussler is pursuing her Masters in Narrative Medicine at Columbia University. She is a third year medical student at the Icahn School of Medicine at Mount Sinai.


