Diana Novaceanu // Throughout the ages, fever has been a constant presence on an individual and collective scale, an “unavoidable part of everyday domestic experience” (Rosenberg, VIII). The concept of fever has been reworked and reshaped with the gradual change of medical discourse. Moreover, fever effortlessly crossed into the metaphorical realm: its distorted sensory perception seemed suited to creativity, genius or madness. It has been tied to heightened emotions or to misery. We become “feverish” for objects or persons of desire. Fever simultaneously binds and separates, as it also epitomizes otherness and menace.
Ancient Greek scholars viewed pyrexia (derived from a term meaning fire) as a disturbance in the equilibrium between humors, with an overlap between it being a sign, a symptom or an affection if its own. Iatrochemistry and iatrophysics experimentation of the Early Modern Era attempted to provide suitable explanations for the overheating of the body, with Herman Boerhaave likening the body’s febrile response to the heat produced in chemical reactions. The advent of the clinic linked fever to the anatomopathological lesion and came to articulate it inside a schema dictated by the emergence of a new sort of medical perception. The growing concern for a healthy social body aided in the emergence of a new type of medicine, centered on epidemics, and would place fever at “the nucleus for modern institutions of public health” (Hamlin, 91). During the twentieth century, fever underwent periods of trivialization and of heightened social and medical response.
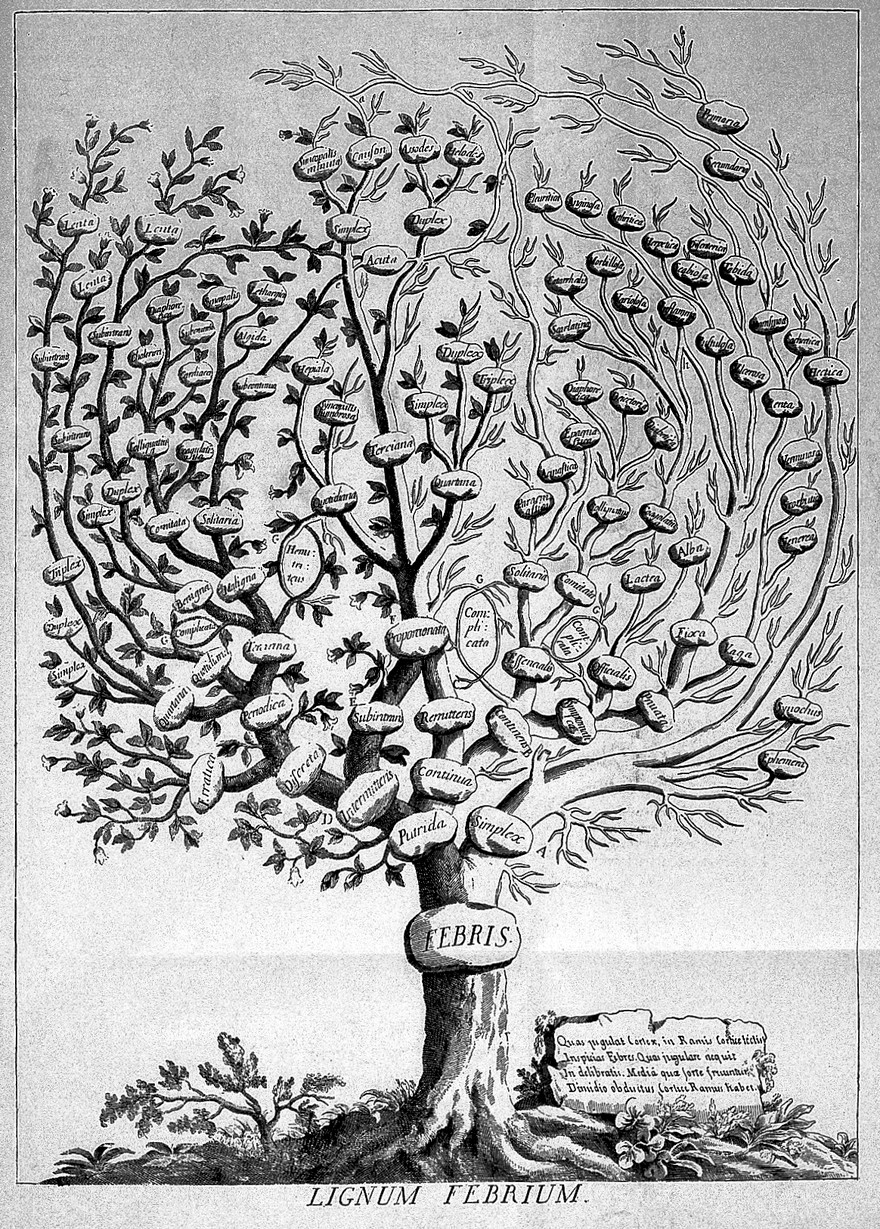
Fever has not altogether lost its bewildering attributes, which have been transfigured and sometimes enhanced in their cultural and biomedical dimension. Febrile illnesses are “varied and extensive” (Cunha, V). Fevers underwent countless classification attempts, being described at times as “putrid, malign, ataxic, or synochus” (Atkins, 284), “intermittent and remittent” (Ogoina, 113), ephemeral, hectic or ardent (Sajadi, 978). The Lignium Febrium, a classificatory tree of fevers from Francesco Torti’s 1712 work Therapeutice Specialis ad Febres Periodicas Perniciosa, displays a corona of complex permutations and inter-dependencies. In the early nineteenth century, chronic fever continued to bypass the “monolithic understanding in Western discourses of medicine and health” (Newby). It was only with the onset of the standardized temperature chart that fever was streamlined and pared down to “the dots and lines that constituted each disease’s signature” (Hamlin, 163).
Febrile conditions may illicit diagnostic dilemmas, preserving their clinical standing as “vexing enigmas” (Cunha, V). Pyrexia of Unknown Origin (PUO) has been outlined as a “persistent fever above 38.3°C (100°F) that evades diagnosis for at least three weeks” (Fernandez, Beeching, 170). The recommended “careful monitoring and exhaustive medical history of the case” depend on collaboration between patient and physician (Cunha, 10). Though patients affected by PUO are often “clinically well enough” to engage in daily life, the lack of a “firm diagnosis” may prove frustrating for both parties and can affect future encounters with the medical establishment. (Fernandez, Beeching, 173).
Fever still evokes a sense of dread, stirring anxious feelings about its implications, especially if the sufferers are children. Over the past few decades, fever phobia has become a talking point in medical and social studies, highlighting the problematic of contemporary fever management. The condition feeds into misconceptions about its effects and associated conditions, such as febrile convulsions. With thermometers and antipyretic medication having become ubiquitous household items, accountability of correct and rightful use came upon parents, particularly mothers. Fever has long been watched over: keeping vigil over a sick or convalescent child is a universal human experience, bridging generations and cultures. The accessibility and relative ease of use of thermometers meant the transitioning of a diagnostic tool outside of the specialized medical gaze. One must learn to assess temperature correctly and decide on a path of action: let the fever run its course or decide to administer medication early on; determine dosage based on the standard recommendations or solicit professional advice; visit an emergency room or an online forum.
The extent of fever phobia raises vital queries concerning the social dissemination of medical knowledge and the ways in which health practitioners are relied on to act. Fever hospitals and fever nurses, for example, had their distinct place in nineteenth and early twentieth century British society. Nowadays, they have been mostly faded out of memory. In the ever expanding culture of medical self advocacy and self management, fever in infants and young children underlines the importance of professional support and reassurance concerning its outcome. One visual iteration may be found in a 1891 painting by Sir Luke Fildes. Entitled The Doctor, it depicts a physician paying a house call to a young patient, as the child’s parents look on. There is admittedly, little clinical material to interpret: none of the medical instruments available at the time are shown and the scene itself bypasses late Victorian class implications. The artist’s first child, a son named Philip, had previously died of typhoid fever, suggesting the depiction of a similar case. The paining attracted critical and popular attention and has been featured in a myriad of medical publications, a testament to the joint vigil between parents and the physician “armed only with his professionalism and perhaps a limited armamentarium of symptomatic reliefs” (Friedlaender, Friedlaender, 3356).
Yet it is in the context of current epidemics and outbreaks that the cultural standing of fever brings forth attitudes and responses that, far from remitting out of the collective consciousness, highlight how it still divides, “by class, place, and sometimes race” (Hamlin, 5). During the nineteenth and early twentieth century, types of fever became associated with certain groups: “prisoners, soldiers, women, Irish beggars, indigenous peoples, and later, with world-historical consequences, eastern European Jews” (Hamlin, 90). Names attributed to febrile diseases may stress the genotypic character rather than their place of origin but they are often addressed using an imperialist and colonialist terminology, “the residuum of a long past” (Hamlin, 6). Exotic locations emphasize the otherness of the disease, whilst holding the “others” accountable for its dissemination.
In the second half of the twentieth century, military metaphors of health and illness would further liken fever to the radar, an internal alarm mechanism, signaling a safety breech or the presence of a foreign agent. Fever denotes “states of abandon and loss of control” (Rosenberg, X). This is evident in the popular culture of pandemics, with fever as a symptom of a zombie transformation and feverish hordes inflicting destruction on an unparalleled scale. Medical facilities are often depicted as overrun hotbeds of infection, posing real life public health implications as “hospitals and isolation centers should be seen as treatment zones to be sought rather than places of death to avoid” (Barret, Brown, 36). At a time when issues such as temperature checks and quarantine are omnipresent topics, an examination of the socio-cultural attitudes to fever, its history and metaphors is necessary for contextualizing what constitutes “perhaps the most ancient hallmark of disease” (El-Radhi, 9).
Header Image: Francisco Torti, Therapeutice specialis: tree of fevers. Wellcome Collection. In copyright
Works Cited:
Atkins, Elisha. (1982). Fever: Its History, Cause and Function. The Yale Journal of Biology and Medicine. vol. 55, pp 283-289.
Barret, Ben. Brown, Peter. J. “Stigma in the Time of Influenza: Social and Institutional Responses to Pandemic Emergencies”. The Journal of Infectious Diseases, no. 197, Suppl. 1. pp. 34-37.
Cunha, Burke A. (2007). Fever of Unknown Origin. New York : Informa Healthcare.
El-Radhi, Sahib. (2011). “The Role of Fever in the Past and Present”.Medical Journal of Islamic World Academy of Sciences 19:1. pp. 9-14.
Fernandez, Cristina. Beeching, Nick J. (2018) “Pyrexia of unknown origin”. Clinical Medicine Journal, vol. 18, no. 2. pp. 170-174.
Friedlaender, Linda K. Friedlaender, Gary E. (2015). “Art in Science: The Doctor by Luke Fildes: Putting the Patient First”. Clinical Orthopaedics and Related Research, vol. 473, no. 11. pp. 3355-3359.
Hamplin, Cristopher. (2014). More Than Hot: A Short History of Fever. Baltimore: John Hopkins University Press.
Newby, Diana Rose. (2018). “Fevered Bodies in Early Victorian Fiction& Medicine”. Synapsis.
Ogoina, Dimie. (2011). “Fever, fever patterns and diseases called ‘fever’ – A review”. Journal of Infection and Public Health, vol. 4, no. 3, pp. 108-124.
Sajahdi, Mohammad M. et al. (2012). Akhawayni and the First Fever Curve. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, Vol. 55, pp. 976-980.
Rosenberg, Charles E. (2014) “Preface”, in Hamplin, Cristopher. (2014). More Than Hot: A Short History of Fever. Baltimore: John Hopkins University Press.


