In healthcare, there has been much debate about the role empathy plays in patient-doctor communication, and whether it can and should be taught to medical students. Narrative Medicine has “not found empathy to be a useful term” and claims empathy to be “a misguided assumption that one can enter into or know another’s experience” (Charon 41). Narrative Medicine offers narrative humility, a framework first articulated by Dr. Sayantani DasGupta in The Lancet, in place of empathy (DasGupta, 2008). DasGupta writes,
Narrative humility acknowledges that our patients’ stories are not objects that we can comprehend or master, but rather dynamic entities that we can approach and engage with, while simultaneously remaining open to their ambiguity and contradiction, and engaging in constant self-evaluation and self-critique about issues such as our own role in the story, our expectations of the story, our responsibilities to the story, and our identifications with the story—how the story attracts or repels us because it reminds us of any number of personal stories.
The philosopher Havi Carel also believes in privileging patient’s voices and their perspective, but takes an approach that is different from narrative humility in arguing for the promotion of empathy. In Phenomenology of Illness, Carel offers a perspectival analysis that is a valuable tool for delineating the relationship between empathy and narrative humility. Carel also develops a useful distinction between the objective body and the body as lived; in other words, the distinction between disease and illness. Carel’s proposal of adopting a second-person phenomenological perspective in order to cultivate empathy appears promising, but it also raises important, unresolved questions about identity and affinity. This essay argues that narrative humility is a better approach, because it avoids notions of mastery while paying attention to affinity and identity.
One of the main tenets of Narrative Medicine is close reading. Readers can examine points of view to enhance our understanding of Carel’s first-, second-, and third-person perspectives (which I will detail below). In telling a story, at the most basic level, there are three possible points of view. When one reads in the first-person, one is reading a story through the eyes/‘I’ of a particular character or narrator. The second-person point of view for the reader is perhaps the most intimate, because the “you” implicates the reader (reading through one’s own eyes/‘I’) in the text and he/she can either accept or reject the implication. The third-person point of view, by contrast, seems to be the most objective, with the “he” and “she” providing a sort of news-quality read. It is at this third-person level where the reader can experience a limited or fully omniscient point of view; there is the possibility of moving beyond the (spatiotemporal) singularity of the first and second point of views.
While Carel does not specifically delve into the literary technique of point of view, it aligns very nicely with her first-, second-, and third-person phenomenological perspectives. For Carel, the first-person perspective is the body as lived; “the body as lived is the…experience of this objective body, the body as experienced by the person whose body it is” (47). This first-person perspective is where one’s illness experience occurs. The experience of a disease is embedded and changes because of the ‘I’. For this thought experiment, we might assume that there are two patients who share the same biological and objective manifestations of the same disease: cancer. Yet if patient A says “I have cancer” and patient B says “I have cancer,” even though the cancer is the same, the experience and perhaps even the treatment will be different, because the ‘I’ is not the same.
Empathy occurs, according to Carel, in the second-person phenomenology of illness. This second-person phenomenology “involves perceiving aspects of what the ill person experiences” (Carel 46, emphasis added). Carel offers the example of when one spouse becomes chronically ill, such that the other spouse becomes limited in what he/she can also do. Thus, the other spouse is also having an illness experience. Carel notes that the kind of illness experience between spouses is different, but she suggests as well that health professionals adopt this second-order perspective towards illness. This second-order perspective, she argues, can be developed through phenomenology, and more specifically a phenomenological toolkit. Carel describes three components of the toolkit:
1. Bracketing the natural attitude toward illness, suspends the belief in the reality of an objective disease entity,
2. Thematizing illness – attending to the cognitive, emotive, moral, or aesthetic aspects of a phenomenon,
3. Taking the new understanding of illness emerging from these two steps, and examine how it changes the ill person’s being in the world.
Carel envisions the toolkit being used in workshop with health professionals and patients, and as one means to address the epistemic injustice that privileges the doctor’s perspective over the patient’s. I agree that health professionals should be receptive to the patient’s illness experience, but I believe that narrative humility is a better approach to achieve this goal.
In Carel’s example, while both partners have a shared illness experience, these experiences are not the same, because the ‘I’ is different. Problems arises when health professionals attempt to adopt second-order perspective of trying to understand a patient’s illness experience, which is nonetheless predicated and dependent on one’s own first-person perspective. In this second-order phenomenological approach, how would one differentiate between true “aspects” of what a patient is feeling and “aspects” of what the clinician is feeling? Furthermore, the couple dynamic of living life together and being bound by a legal document does not apply to the patient-doctor relationship. Patients and doctors are not couples; the relationship is inherently asymmetrical. Meanwhile, while helpful, the practices of the phenomenological toolkit do not answer questions about differentiation and projection of the self. Bracketing the natural attitude is helpful in allowing doctors to think more about the illness experience than the disease, but how does this translate into feeling and empathy? Thinking is still a cognitive and disembodied practice. Furthermore, Carel cites elsewhere the disability paradox — those without X condition overestimate the impact of X condition on the quality of life of those with X condition — as proof that there is not a correlation between well-being and disease processes. This overestimation, however, can result not only from conflating disease and illness, as Carel suggests, but also from not having first-person experience of the patient’s condition. Similarly, in thematizing, “attending to the cognitive, emotive, moral, or aesthetic aspects of a phenomenon,” overestimation is a potential problem (200).
As a forum for cultivating a second-person phenomenological perspective, Carel proposes a mixed workshop of patients and health professionals to thematize illness. In this workshop, Carel writes that “The patient may thematize her illness primarily emotively, while a health professional will thematize it cognitively” (200). While mixing such perspectives would encourage a more dynamic, nuanced understanding of illness, I feel that such a workshop would fall short of cultivating a second-order phenomenological or embodied approach, if on the one hand, patients are primarily using emotions, and on the other hand, if physicians are (scientifically) thinking about illness. And identifying patients strictly with emotions also risks trivializing their perspectives and reifying the institutional hierarchy the workshop is intended to challenge. Carel offers space for physicians to explore and use unnamed emotions triggered by “visual and sensual samples” in order to understand illness and how it changes a person’s being-in-the-world. But the practitioner again runs the risk that emotions are triggered because of some resonance and relation between the samples and the self. In this hypothetical workshop, Carel does write that a family member might thematize illness as an experience of empathy. This makes sense, in that it is similar to Carel’s example of the couple’s shared illness experience. For health professionals this appears to be more difficult due to the asymmetrical relationship.
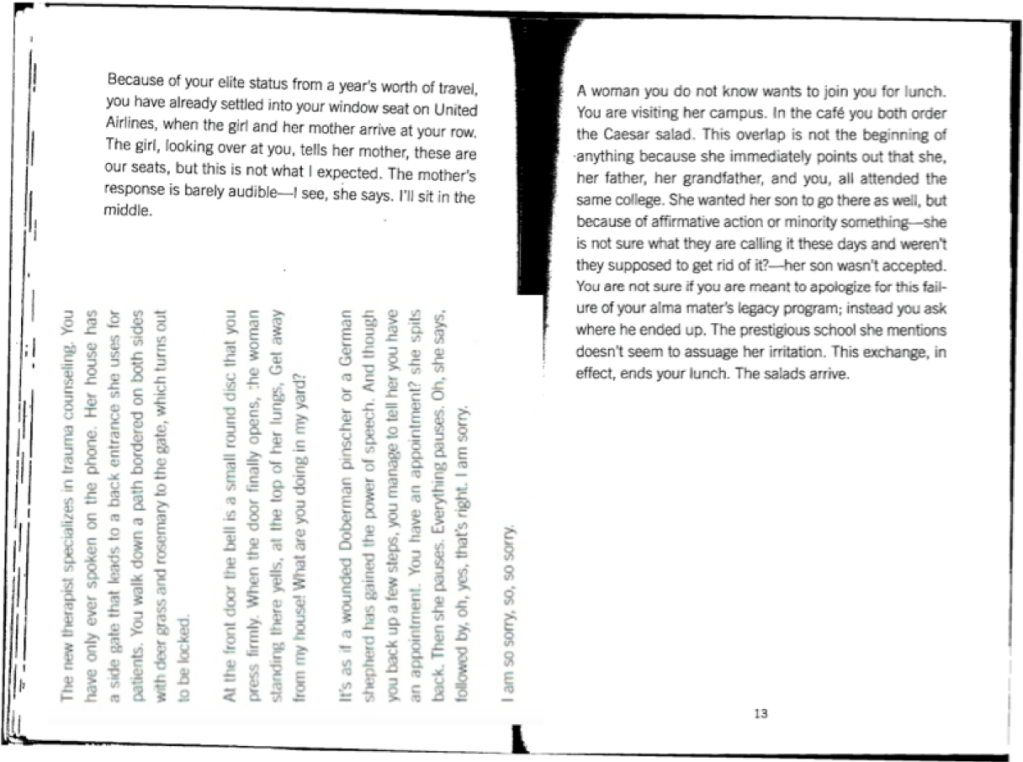
In my own professional experience, I have found that using the second-person perspective as a mode of empathy can be problematic. During a Narrative Medicine workshop that I led, with Post-Baccalaureate students at Columbia, we looked at one piece written in the second person. The piece we looked at were excerpts (Figure 1) from Citizen, by Claudia Rankine. Each excerpt contained a scenario of a micro-aggression in which the “you” was experiencing the micro-aggression. The class consisted of ten white women, one black woman and one black man. I appreciate the activist nature of Rankine’s work, but for the purposes of the class, we were able to consider its shortcomings in terms of promoting empathy in the reader. Whereas the white students felt simultaneously outside the text and accused because of the implied context suggesting that the “you” was a person of color and the “I,” “the woman,” “the mother” etc. a white person, as a person of color I did not feel accused but instead could imagine myself as the “you” in the specific situations. Rebecca Garden writes in “The Problem of Empathy”:
The problem of empathy begins with the preoccupation with self that obscures the other. Empathy depends on the experiences and imagination of the person who is empathizing, and this dependency has the potential to obfuscate or exclude the patient’s suffering and the meaning the patient makes of suffering. (555)
The problem with promoting empathy is that it depends on the self and the self’s past memories, experiences and intersectional identities. Empathy also depends on affinity. Whereas in Carel’s example, a couple has a close affinity with a shared life and projects, the white students in the class were revealed to have a distant affinity, because they have a very different life and orientation toward the world than people of color. However, my experience with the text also illustrates the danger of empathy. As a black person who has experienced micro-aggressions, I felt a very close affinity to the scenarios in Citizen. Garden writes:
Halpern argues that physicians should imagine “how it feels to have a certain illness, disability, or psychological injury.” Recommending that physicians use pronouns such as ‘I’ and “he” interchangeably, Halpern enables appropriation of the patient’s experience through subject positions. (Similarly, Spiro claims that empathy is evident when “‘I and you’ becomes ‘I am you,’ or at least ‘I might be you’”). (557)
By thinking that I could empathize with the character in the text because of our shared identities and subject positions, I was in many ways appropriating the experience of the person who actually was the recipient of the micro-aggression. It is easy to forget the “not the same,” such that the “I might be you” becomes “I am you.” Thus, while a text does not correlate to a patient, I wish to suggest through this lived example that one can still see how adopting a Carelian second-person perspective toward illness in the name of cultivating empathy also risks collapsing the provider’s perspective into the patient’s. This is avoided with a narrative humility approach.
Narrative humility is having the understanding that a patient’s story belongs to him or her. While physicians can certainly co-create and co-construct a narrative with a patient, the difference between narrative humility and empathy revolves around control and power. In empathizing, a physician is controlling the degree (implicit or explicit) of emotional investment. But in narrative humility, the physician understands that they can never fully know the story of a patient. What is the reason behind this humility? Giving an Account of Oneself, by Judith Butler, a foundational text in the field of Narrative Medicine, provides the answer. Butler argues that there is an “opacity of the self”: if we cannot give an entire account of our own beginning how can we expect the same from others? Carel’s solution to poor patient-doctor relationships is for doctors to gain a new understanding of illness and privilege the patient’s perspective through the phenomenological toolkit. Physicians might have access to parts of the first-person perspective or illness experience through first-person reports, but physicians can never fully know the patient’s reality, because certain experiences are inexpressible and contain some manner of opacity. But if physicians adopt narrative humility — recognizing their own opacity, rather than employing a competency-based means of gaining a second-person phenomenological insight into the experience of illness — we might produce more reflective doctors who value the patient’s perspective.
Marcus Mosley is a third-year medical student at The City University of New York (CUNY) School of Medicine, who is currently conducting research examining the presentation of race in the medical curriculum. Mr. Mosley has a master’s in narrative medicine from Columbia University.
Works Cited
Butler, Judith P. Giving an account of oneself. Fordham Univ Press, 2009.
Carel, Havi. Phenomenology of Illness. 2016.
Charon, R. The principles and practice of narrative medicine. Oxford University Press, 2017.
DasGupta, Sayantani. “Narrative humility.” The Lancet 371.9617 (2008): 980-981.
Garden, Rebecca E. “The Problem of Empathy: Medicine and the Humanities.” New Literary History, vol. 38, no. 3, 2007, pp. 551-567.
Rankine, Claudia. Citizen: An American Lyric. Penguin Books, 2015.


