My toddler’s cough wakes me in the night — the sound has a quick attack, starting like a bark, and an abrupt end, like a choke — triggering my adrenaline. This gasp in the dark warrants a call to the pediatrician’s office. I rush into his room to get him to sit up and drink some water and listen closely to his raspy breathing. His barking cough continues in fitful bursts like a compulsive hiccup interrupting every breath. I pause for him to heave and wretch but nothing comes — just a startling silence, a temporary suffocation, at the end of the cough. This must be the croup I read about.
In my mind’s eye, I see Ruth’s daughter, little Daisy, dying of croup in her mother’s arms: the poor babe suffocates by the fireside in Sarah Parton’s Ruth Hall (1862) in a chapter gloomily titled, “The Old Doctor Arrives Too Late:”
The strong fire-light fell upon Ruth’s white figure, as she sat, pale and motionless, in the corner, with Daisy on her lap, whose laborious breathing could be distinctly heard in the next room. A dark circle had settled round the child’s mouth and eyes, and its little hands hung helplessly at its side. Dinah was kneeling at the hearth, stirring a fresh mustard paste, with an air which seemed to say, “it is no use, but I must keep on doing something.”
(Hall 49)
Ruth, who has been pacing all night long like a ghost, is attuned to her daughter’s shrill cough and her every sound. That invisible cord that tethers our hearts to our children, whether born of us or adopted, can never be cut.
Sarah Parton was a controversial figure: both a mother and the country’s most highly-paid newspaper columnist whose biting satire spared no one, especially when it came to injustices against women. Ruth Hall tells the story of a white, middle-class woman who starts out as a naive housewife. After facing various tragedies and obstacles (spoilers: her husband dies, leaving her in debt and her in-laws and family refuse to help, so she must take up work in a society where there are no jobs for widowed women with children), she transforms into a self-made, economically independent newspaper columnist like the author herself, who wrote under the gender-neutral pen name “Fanny Fern.” Even in this early scene above, I know what Ruth is capable of and I trust her intuition is sound, especially when it comes to her daughter, Daisy.
Ruth is the rare nineteenth-century mother I have long admired because she is so authentic and unpretentious: she climbs fences to collect wildflowers with Daisy—their living room “has the fragrance of a green-house”—and she lets her kid be a freaking kid. The nursery “is strewed with play-things…a broken doll; a torn picture-book…a few acorns; a little red shoe, full of particolored pebbles…” (Hall 35-36). Unlike the typical corset-squeezed wife, Ruth isn’t afraid of a bit of mess and she’s in tune with her children, immerses herself in whatever fascinates them, a little more like the mom I’ve always wanted to be.
I study my son’s chest to watch him breathe like I did when he was a newborn.
My baby taught me how to care for him by cultivating in me what I would now call a sound intuition — what Donna Haraway calls a “situated knowledge” particular to my specific experience listening and observing him over the years as he grew (Haraway). Postpartum I used to sit at his cribside and find peace watching each heave of his breast while he slept. An infant offers such earnest utterances. My whole body responded to his every murmur and motion.
Those early, unassuming infant howls are sweet — and yet powerfully disarming, making my chest prickle to ready my breasts to produce the desired milk. As his cries became more distinguishable to me, I became his translator for others: “He needs burping;” “Oh, that’s just gas;” “He needs to sleep;” “Time for milk.” Now I translate his toddler language for others: “He’s telling you he wants to do it himself;” “He’s asking for water;” “He just needs some snuggles.”
What is the nature of a sound intuition? Some of it is knowing the context of a situation, some of it is prior bodily experience (that my lizard brain responds to my child’s signals), and most of it is deep listening. Deep listening means being truly present in a moment, allowing yourself to be still and take in all the cues, heard or otherwise, being given. I happened to breastfeed but that’s only a part of it: much of my intuition as a parent comes from paying attention to the nuances of sound, learning my child’s pitches and tones, the difference between whining — like a cat’s meowing for food — and a real crisis that makes me drop everything and run. As a sound studies scholar who follows the research, I know this has nothing to do with a “mother’s intuition,” which is an unnecessarily and incorrectly gendered phrase. As a result of the neural pathways that change when a child becomes your charge, any primary caregiver of any sex, gender, or relation to the child (biological, adopted, etc.), acquires an attentive ear, a sound intuition. And it can’t be undone (Feldman 2015; Feldman 2017).
Dinah, a black maid in Ruth’s house, is the only character in Ruth Hall who diagnoses Daisy swiftly and correctly. In “Dinah’s Warning,” the chapter before the grim fireside scene above, Dinah persuades Harry (Ruth’s husband) to send for the doctor. The doctor (Harry’s father) has been neglectful and dismissed the parents’ earlier calls for help—he has not listened nor treated Daisy’s illness seriously.
Dinah’s character may be based on Harriet Jacobs, the mother of two and author of the fugitive slave narrative Incidents in the Life of a Slave Girl (1861). She worked as a nursemaid in Parton’s brother’s household and was one of the few who didn’t abandon Parton when her second husband defamed her. When Jacobs was able to bring her children North, Parton took her daughter, Louisa, in and reportedly treated her like she would any houseguest or a member of her own family: “Louisa entered into all of the social activities of the family…dining, playing games, going for walks, visiting neighbors” (Warren 224).
Parton depicts Dinah as a knowledgeable housemaid; it is Dinah who warns Daisy’s cough is a death sentence. When Harry says the doctor will be there in the morning, she points at Daisy and whispers to him, “She won’t.” Dinah is right but cursed by others’ disbelief, like Cassandra in Greek mythology. Reading her today calls to mind the childcare crisis and the numerous women of color providing care who face the immense challenges of systemic racism and sexism that make them feel undervalued and pressure them to overwork to combat prejudice (Oldham). Parton’s depiction of Dinah grants her a respected role in the family but her dialect is jarringly racialized, which suggests why Dinah’s voice isn’t heard sooner in the novel. Parton draws heavily on the mammy stereotype when she writes from Dinah’s point of view, revealing the limits of her sound intuition to cast a genuine Black female authoritative voice. Dinah urges: “Don’t you know, Massa, it’s de croup! de croup! de wu’st way, Massa! Oh Lor’ !” Eventually, at this point, Harry becomes alarmed, finally heeds her advice, and races to harness his horse “in an instant” (Hall 47).
An “instant” today can be as short as a phone call to the pediatrician and as long as the wait time for a response. Tonight is the first time I wake up knowing we will call the doctor’s office. My son’s breathing sounds labored and raspy and the cough is too suddenly stifled. Was that the sound of his trachea closing? My body’s affective response says, this feels wrong. I leave a message on the emergency line and wait for the on-call doctor to get back to me. While comforting my son, I’m giving orders to my partner: turn on the humidifier, get the eucalyptus essence, we need more water. I examine my son again: he’s lackadaisical but responsive.
A missed call.
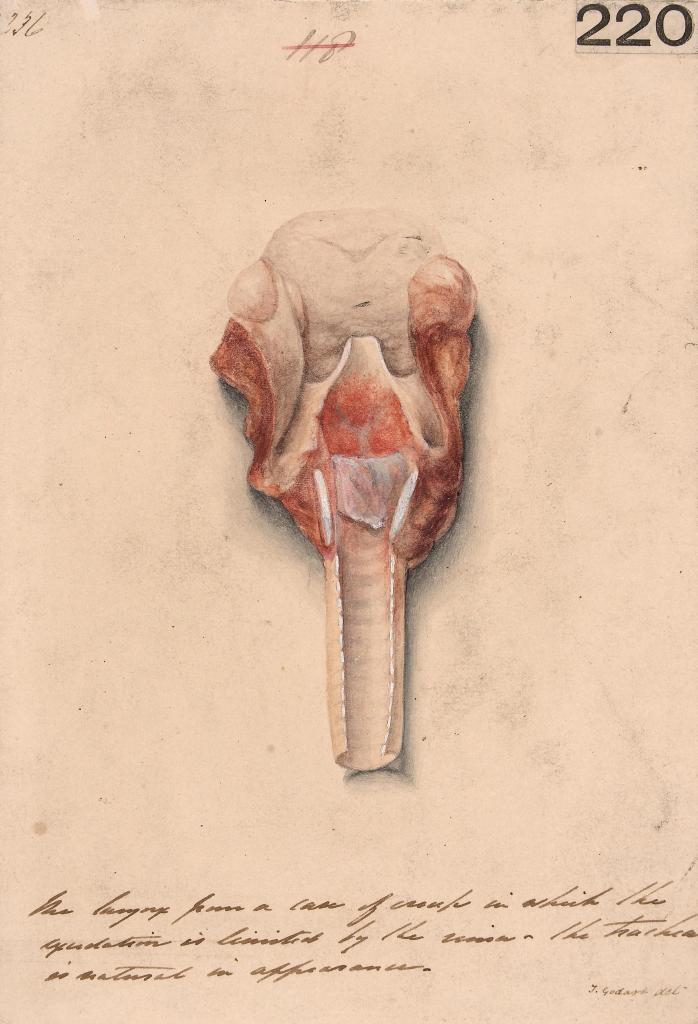
In an 1848 issue of The New York Journal of Medicine, croup is described as an “almost universally fatal malady.” The article on “Croup, or Laryngitis Membranacea” notes that — when the “disease [i]s confined to the tonsils, glottis and larynx” — treatment of inflammation (with silver nitrate) is “not only feasible but justifiable from the first.” However, when it descends into the trachea, bronchia, and lungs, “little if any good can result.” The article emphasizes the importance of early intervention: “our readers will readily recognize the propriety of early resorting to the treatment.” Later, Dinah matter-of-factly accuses the doctor of murdering both mother and child by delaying so long to come to the house (Hall 49). If only they had known in Ruth Hall to simply open the window to let in the winter air.
Both primary caregivers in Ruth Hall — Daisy’s birth parent and housemaid — exhibit sound intuition. The first indicator of Daisy’s illness is a cough on a cold day, and no one seems concerned. (The underlying cause likely would have been any one of the viruses that can lead to croup before the age of three, when the trachea is still dangerously narrow in little ones.) Later, during the night, Daisy’s cough worsens, waking Ruth, and Ruth’s pacing about the room wakes her husband, Harry. She says, “listen to Daisy’s breathing; it sounds as if it came through a brazen tube. She must be ill” (Hall 43). Rather than attend with the same sensitive ear, Harry patronizes Ruth, calling her “a frightened little puss” (44).
Unfortunately, the burdens of childcare are still largely shouldered by women. The phrase “mommy brain” is often used to describe the neural rewiring that happens in the brain of a primary caregiver in those early days of infancy. Some of the rewiring happens to our listening. Research has shown improvement in a birth parent’s hearing postdelivery (Kwatra, et. al.) but this phenomenon isn’t limited to just the birth parent. Dr. Ruth Feldman explains her extensive research in the recent documentary Babies (2020): whoever takes on the role of the primary caregiver—no matter their gender or relation to the child—this person becomes more sensitive to their baby’s sounds and this sensitivity is permanent, as is the rewiring of the brain.
In Parton’s Ruth Hall, Daisy’s primary caregiver cannot sleep through her daughter’s coughing and, though she second-guesses herself — “Perhaps her fears were groundless, and she was over-anxious” (Hall 44) — she eventually asks Daisy, “What is it, darling?” and Daisy grasps her throat with both hands and replies, “It hurts” (44). Ultimately, Ruth’s intuitive affective response wins: she rouses Harry again to send for the doctor. The doctor dismisses Ruth’s concerns as needless fussing, gives them a small bottle of medicine without leaving his house, and says he will come in the morning.
How do we know when an intuition is sound? There is a humanistic element of caregiving in literature that reminds us to observe and listen closely. Ruth Hall asks her child questions and listens in an active dialogue. Although she lacks the training to diagnose Daisy, she does what she can to examine her, “marking every contortion of feature, noting every change of posture” (44) to sense something is awry and determine professional attention is required. Parton’s scathing portrayal of the doctor points to the importance of listening in making a diagnosis, and highlights the humanistic element — namely, the two-way communication between caregiver and patient — in intuitive caregiving, which this fictional doctor lacks. (Note: the character is based on Parton’s father-in-law, who she satirizes as an unfeeling hypocrite — suffice it to say, she had good reason to be bitter.)
As Parton well knew when writing Ruth Hall, a male-dominated society has traditionally dismissed and ignored the fears of primary caregivers, 94 percent of whom are women and 40 percent are people of color today (Oldham), and patronized them — like Dinah, a black woman with many years of house and nursemaid experience, and Ruth, a parent who knows her own child’s sounds better than anyone else.
My phone rings.
Our pediatrician has tried and tried again to call me back, clearly sensing something is amiss, and eventually overcomes bad cell reception. The doctor asks me to hold up the phone to my son’s mouth so he can listen to his breathing, and for a moment – 15 seconds or so – everyone becomes still and listens. Can you hear it too? The doctor confirms my suspicion that it’s croup and suggests a common remedy for children’s colds: bathroom steam to ease the cough. We try this, and the coughing fits return. My son shakes his head, too worn out for tears, and pleads, “No shower.”
My enemy is the summer heat. I remember Daisy by the fireside.
I’ve heard wintertime stories of croup cough from friends who became parents before me — what could have been horror stories in the 19th century can end well now. Stories are such a valuable aural inheritance. When these women took their children outside to get in the car and go to the emergency room, the shock of cold air reduced the inflammation and, upon arriving at the ER, their children were already in a better state. This knowledge of croup, and the wisdom in exposing children to cold air instead of heat for treatment, has been passed among primary caregivers for some years now. Sarah Parton, through her novel Ruth Hall, imparted some of her sound intuition to me: I knew to pay attention to these stories, to ask and be curious about the ghastly bark of croup, because I had read this novel ten years ago and wondered at the sound.
As a parent, I feel at a loss for answers more times than I care to admit. For me, a sound intuition is a daily practice of listening and being curious so my ears and mind are open. Diagnosis arises out of an exchange between caregiver and patient. I listen to my son’s pleas and turn off the hot running water to stop the warm steam, get my eucalyptus essence and cool mist from the humidifier going, and I turn the air conditioning down to 67, telling myself I am not a bad parent for blasting my sick child with cold air. In early June, it is hard to believe summer is already here; it’s oppressive even on some nights in humid New York.
The next day, going outside in the sun for 10 minutes makes my son’s cough worse enough to warrant a follow-up sick visit to the pediatrician’s office. This time the doctor suggests opening the freezer door and letting him breathe in the cold air. She also gives us a steroid and the croup goes away in less than two days.
I had never heard a croup cough first-hand, only in Ruth Hall and friends’ stories, and I always wondered at “Daisy’s shrill cough.” A friend once told me, “When you hear it, you’ll know.” If not by the sound itself, I knew it from the intuitive fear that woke me in the night.
Bibliography
“Croup, or Laryngitis Membranacea, Treated by the Use of Argenti Nitras.” The New York Journal of Medicine, vol. I, no. I, 1848, p. 94–95.
Feldman, Ruth. “The adaptive human parental brain: implications for children’s social development.” Trends in Neurosciences, vol. 38, no. 6, June 2015, pp. 387–99.
Feldman, Ruth. “The Neurobiology of Human Attachments.” Trends in Cognitive Sciences, vol. 21, no. 2, February 2017, pp. 80–99.
Haraway, Donna. “Situated Knowledges: The Science Question in Feminism and the Privilege of Partial Perspective.” Feminist Studies, vol. 14, no. 3, 1988, pp. 575–99.
Kwatra, Devanshu, et al. “Can Pregnancy Lead to Changes in Hearing Threshold?” Ear, Nose & Throat Journal, vol. 100, no. 3, June 2021, pp. 277–80.
Oldham, Cheryl. “Childcare Providers—Especially Women of Color—Need Our Support. Here’s How We Can Help.” U.S. Chamber of Commerce Foundation, 1 March 2022.
Parton, Sarah Payson. Ruth Hall: A Domestic Tale of the Present Time with Other Tales. (Halifax: Milner and Sowerby, 1862).
Warren, Joyce. Fanny Fern: An Independent Woman, Rutgers University Press, 1994, pp. 223-24.
Image: Godart, Thomas. “Larynx from a case of croup.” St Bartholomew’s Hospital Archives & Museum. Attribution 4.0 International (CC BY 4.0)


