David Robertson //
‘Suicide rate up 33%’ reads a recent news headline; ‘dementia skyrocketed by 117% over just 26 years’, reads another.[1] Internationally, health media today indicates a growing reliance on the quantitative representation of health findings, outcomes, and interventions in a display of what philosopher of science Ian Hacking once described, referring to the statistical knowledge newly valued by nineteenth-century European states, as an ‘avalanche of printed numbers.’[2]
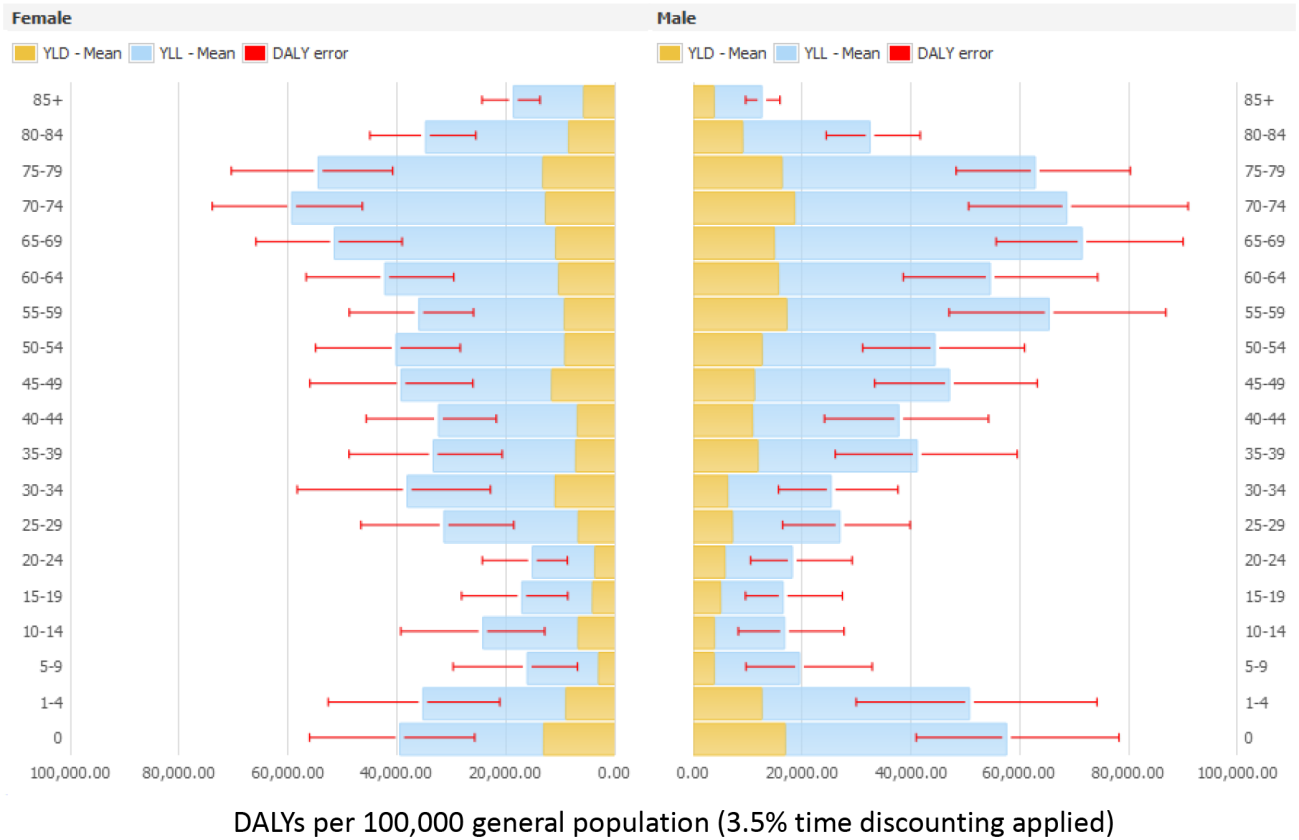
Nowhere is this reliance more evident than in the burgeoning field of global health. Increasingly, quantitative data – or what, in its effort to make commensurable data from different times and places, may more accurately be referred to as “metrics” – have come to play a central role in channeling global health interventions. Take the DALY (disability-adjusted life-year), developed in the 1990s as a means of measuring the burdens of different diseases or disorders, for example. The World Health Organization describes the calculation of the DALY as
the sum of the Years of Life Lost (YLL) due to premature mortality in the population and the Years Lost due to Disability (YLD) for people living with the health condition or its consequences[.]
Or, in mathematical terms, ‘DALY = YLL + YLD.’[3]
Such metrics can undoubtedly offer a valuable means of assessing health situations and making decisions about where best to intervene. However, like any instrument for measuring and intervening in the complex texture of the world, they have both intended and unintended consequences which influence the kinds of knowledge that come into sight. Three “Cs” indicate some of the ways in which metrics have shaped the field of global health: commensurability, circularity, and commercialization.
Commensurability: In Trust in Numbers: The Pursuit of Objectivity in Science and Public Life (1995), historian Theodore Porter argued that quantification ‘minimizes the need for intimate knowledge and personal trust’ between scientists and, thereby, helps science construct a global network beyond local research communities.[4] Turning the local into a figure that can be successfully exported elsewhere requires the production of good numbers. Claims of commensurability are at the center of what being a “good” number is, allowing claims made in one place to be confirmed or questioned elsewhere.
Yet perfect commensurability is always out of reach. The production of global health data often requires making less rigorous data collection practices such as population surveys commensurable with more reliable data gathered in countries which have more substantial health infrastructure. Where such data cannot be reliably produced, the demand for numbers produces a further mathematical move; modelling.
Take, for example, the use of the “sisterhood survey” to calculate maternal mortality metrics for sub-Saharan Africa. Undertaken each five to ten years, the surveys rely on research assistants surveying a sample of people regarding the deaths of siblings. As scholar Claire Wendland writes:
If a dead sibling was a sister and at least twelve years old when she died, the interviewer asks whether she had been pregnant at the time or within two months of death. The survey respondents’ responses, as recorded by field surveyors, are then weighted and extrapolated by statisticians to represent the nation.
These less-than-certain survey extrapolations then become one of several factors, such as changes in the country’s GDP, in a model attempting
to compensate for suspected under- or overreporting, throw out data deemed too far off to be plausible, impute data where none are available, and estimate uncertainty ranges of both deaths that are counted and death rates that are imputed.[5]
In nations where no count has been made in the first place, the strive for commensurability can produce a second “C;” circularity. Wendland cites the example of Equatorial Guinea which in 2010 showed an impressive decline in maternal mortality figures despite the fact that no count of maternal mortality had been made for over twenty years. This finding was the result of statistical modelling which, among other things, factored in the country’s impressive growth in GDP as one substitute for the lacking health survey data. Like the other five factors making up this model, none were direct counts of the health situation, but rather, estimates used to get around the lack of such hard data.[6] In other words, the production of numbers about people was facilitated through the production of numbers about other numbers.
The irony of the circularity problem is that the lack of the very infrastructure required to produce durable data in the first place leads to a greater reliance on the substitution of such data with modelled metrics. In an international health landscape which has been importantly shaped by the structural adjustment policies of international financial institutions of the 1980s and nineties, metrics offer a means of obtaining health information in areas where such data are scarce due to the erosion of state health infrastructure.
The era of post-structural adjustment policies brings us to the final “C;” commercialization. One important driver of the rise of global health metrics is the ongoing insertion of international health into financial markets. As the field of global health has expanded there has been a concomitant rise of investment in global health sectors. While previously largely limited to the pharmaceutical sector, investment in areas that used to be conceived as public health domains continues to grow and is driving an increasing reliance on metrics as the sine qua non of accountability. The Bill and Melinda Gates Foundation, founded in 1999, has been at the forefront of investments in public-private partnerships prioritizing a logic of financial accountability. Accountability to this standard is largely measured using new metrics like the DALY, which just-so-happen to fit the forms of reasoning of financial investors looking for potentially profitable investments.[7]
Metrics are not, of course, a financial conspiracy against the global poor. However, as a means of summarizing health problems and outcomes and holding recipients accountable, they are more amenable to financial investors than other forms of representation. Moreover, as future funding is linked to metrics through accountability, obtaining “good” numbers can become a leading priority, thereby displacing other healthcare priorities. As Vincanne Adams has written:
Increasingly, doing good global health means setting up one’s intervention as a laboratory study in which the ability to get good data – of sufficient quality, sufficient quantity, and demonstrating fidelity of method – matters as much if not more than the health problem that is being studied.[8]
Like any other instrument put to use in the pursuit of health, metrics can offer valuable insights into the spread of the global burden of disease. But when we look past the numbers at the much messier and mundane nature of their production, we see that this surface precision conceals a much more complicated picture. ‘It is when we fail to recognize them as partial, created, fallible stories’, writes Wendland, ‘that the metrics of global health are especially troubling.’[9]
Featured Image: Burden of Six Healthcare-Associated Infections on European Population Health: Estimating Incidence-Based Disability-Adjusted Life Years through a Population Prevalence-Based Modelling Study – Scientific Figure on ResearchGate. Available under Creative Commons Attribution 4.0 International
Works Cited:
Adams, Vincanne. “Metrics of the Global Sovereign: Numbers and Stories in Global Health.” In Metrics: What Counts in Global Health?, edited by Vincanne Adams, 19-54. Durham: Duke University Press, 2016.
Hacking, Ian. The Taming of Chance. Cambridge: Cambridge University Press, 1990.
Porter, Theodore M. Trust in Numbers: The Pursuit of Objectivity in Science and Public Life. Princeton: Princeton University Press, 1995.
Storeng, Katerini T., and Dominique P. Béhague. ““Guilty until Proven Innocent”: The Contested Use of Maternal Mortality Indicators in Global Health.” Critical Public Health 27, no. 2 (2017): 163-76.
Wendland, Claire L. “Estimating Death: A Close Reading of Maternal Mortality Metrics in Malawi.” In Metrics: What Counts in Global Health, edited by Vincanne Adams, 57-81. Durham: Duke University Press, 2016.
[1] https://www1.cbn.com/cbnnews/us/2018/november/suicide-rate-up-33-percent-franklin-graham-says-people-need-hope; https://www.dailymail.co.uk/health/article-6487695/The-global-map-dementia-Scientists-reveal-memory-robbing-disorder-skyrocketed-117.html
[2] Ian Hacking, The Taming of Chance (Cambridge: Cambridge University Press, 1990), pp. 35-36.
[3] https://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/
[4] Theodore M. Porter, Trust in Numbers: The Pursuit of Objectivity in Science and Public Life (Princeton: Princeton University Press, 1995), p. ix.
[5] Claire L. Wendland, “Estimating Death: A Close Reading of Maternal Mortality Metrics in Malawi,” in Metrics: What Counts in Global Health, ed. Vincanne Adams (Durham: Duke University Press, 2016), p. 66.
[6] Ibid., p. 70.
[7] Katerini T. Storeng and Dominique P. Béhague, ““Guilty until Proven Innocent”: The Contested Use of Maternal Mortality Indicators in Global Health,” Critical Public Health 27, no. 2 (2017): 167.
[8] Vincanne Adams, “Metrics of the Global Sovereign: Numbers and Stories in Global Health,” in Metrics: What Counts in Global Health?, ed. Vincanne Adams (Durham: Duke University Press, 2016), p. 33.
[9] Wendland, p. 79.