Kamna Balhara // Among the many upheavals that medicine has faced in the 21st century, few changes have inspired as much conversation and controversy as the widespread implementation of the electronic health record (EHR). While some physicians see its general adoption as a sign of progress, many view this spread as a metastatic process that encroaches upon key elements of patient care and physician identity. This post will cover one facet of an ongoing analysis of physicians’ texts on the EHR, specifically focusing on storytelling and narrative. Physicians have written extensively on how the EHR destabilizes our own rapport with patients’ stories; this narrow view, however, risks obscuring the transformative ways in which patients may be breaking new narrative ground in the EHR era. This post will suggests the potential for physicians and patients to jointly navigate and circumvent the reductive confines of the EHR as a space of shared narrative control.
Medical record keeping is no stranger to significant changes in both form and function, having evolved from didactic case histories inscribed on papyrus in antiquity, to archival case books in the 19th century, to official hospital record at the dawn of the 20th century.[1] In 2009, the EHR was established as the definitive modality for medical record keeping in the United States after the passage of the Health Information Technology for Economic and Clinical Health Act (HITECH). Prior to HITECH, only 17% of American physicians were using EHRs, along with 9% of hospitals.[2] By 2017, almost all hospitals and nearly 80% of office-based practices were using EHRs.[3] This meteoric growth has engendered significant discussion among physicians in both popular and scientific media.
A common thread in physicians’ critiques of the EHR is a collective sense of loss of the physician’s identity as storyteller. The keeping, collecting, and telling of patients’ stories is described by multiple physicians as an essential aspect of clinical practice.[4-7] Some commentaries, however, describe how as the handwritten chart has gone extinct, the EHR has erased the storyteller’s visual signature. The EHR’s rigid confines also homogenize the physician’s individual narrative voice and style. Concerns about “templated notes,” “the tyranny of clicks and auto-populated fields,” “blanks on our screens,” “drop down menus, cut-and-paste text fields and lists,” “answer boxes,” and “boilerplate entries” populate many physician concerns about the EHR.[5, 6, 8-11] The result is the loss of “independent, personal” expression.[6] The physician’s written expression is made uniform, one indistinguishable from the next.
The content, too, becomes the same, as narrative control is relinquished to the machine. There is a perception among physicians that the only story produced through the EHR is the same story repeatedly. Rosenbaum references an anecdote of a physician who once used his notes to distinguish one patient from the next, but he now feels as though he “never saw them before” and “can’t even picture their faces.”[5] Patients must be labeled via problem lists and diagnoses from drop-down lists that dictate these choices. These menus, for instance, offer diagnosis codes from the International Statistical Classification of Diseases and Related Health-Problems, which have grown in number from 14,000 in a previous iteration to 69,000 in their current form. As the labels offered by the EHR grow increasingly granular, they lose their ability to illustrate or communicate a meaningful bigger picture.
Meanwhile, beyond feeling that the physician’s power as a storyteller in meaning-making is challenged, some also fear a loss of authenticity and accuracy. The time-consuming nature of the EHR leads to the search for shortcuts, including content-importing technologies, such as copy/paste, templates, or macros that allow for insertion of pre-set text. Physicians describe how notes are now populated with “misleading inaccuracies or fraud.”[9] “Disease labels” for instance, “[are] immortalized by being cut and pasted… so that by sheer repetition, a whiff of tricuspid insufficiency turns into a raging torrent.”[4] Against this backdrop, words are perceived to have lost their connection with understanding and meaning. [5]
Many such physician commentaries frame the physician-EHR dynamic as that of a duo, be it an uneasy partnership or dyadic rivalry. What this approach misses, however, is that there is another party that must be considered in this conversation: the patient. [1] “The Note lives on in the voice of the machine,” writes one physician.[7] Yet this “machine” may also permit another voice to enter the note, that of the patient. The voice of the patient has always existed in forms such as popular media and literature, but has been, until now, largely silent within the medical record. While verbatim quotes from the patient are sometimes documented in the “chief complaint” section of a chart, the verbal narrative relayed by a patient during an encounter disappears under layers of paraphrasing, selectivity, and medical jargon. However, the EHR has the potential to generate space for patients to inscribe their own narratives within the official records of the healthcare system. In forcing the physician to vacate the role of sole arbiter of the patient narrative in the medical record, the EHR has, perhaps unwittingly, created space for the patient to step in. Applied correctly, the EHR may have the potential to restore some narrative control to patients via generating power to both access the narrative and create the narrative.
I do not wish, here, to extol the values of the EHR or excuse its failings. There are very real concerns regarding the impact of the EHR on patient-physician relationships, physician wellness and engagement, quality of care, and privacy. Moreover, there is as yet insufficient data on its safety. But I would like to broaden the scope of the conversation by exploring where physicians and patients intersect with narrative in the EHR era. Much of the conversation on the EHR itself has also been dictated by and focused upon physicians; the patient-EHR relationship warrants further exploration.
In the EHR era, there is potential for greater patient engagement with narratives and with personal health information, both within the physical confines of the clinical encounter and without it. Luke Fildes’ painting of “The Doctor” (1891) has frequently appeared in physician commentaries and across social media as an aspirational, if somewhat antiquated, image of a physician wholly engaged in the care of his patient.
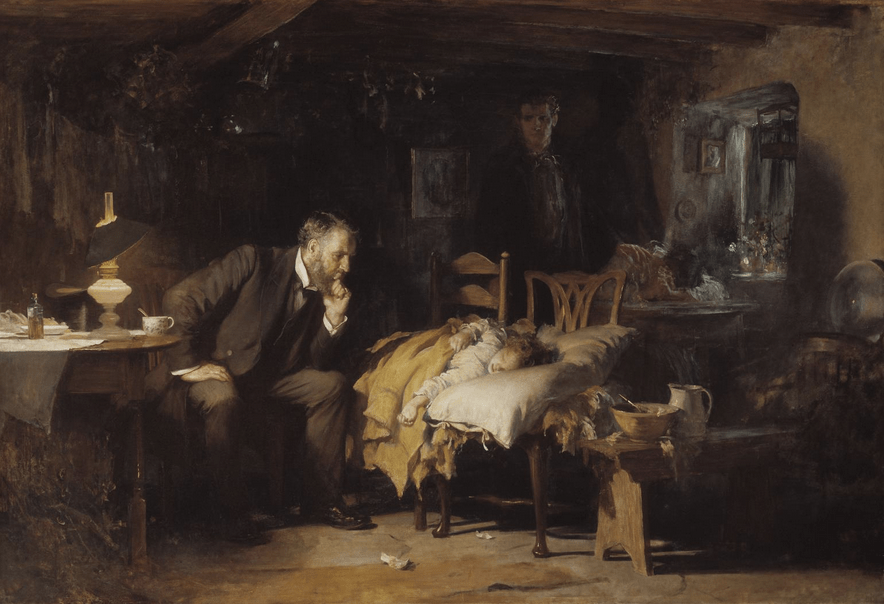
This image is often contrasted with the stereotype of the EHR-era physician whose attention is instead riveted to the computer screen. In Fildes’ image, however, neither patient nor parents engage in any active dialogue in the encounter. The patient is an inert form, with the caregivers literally painted into the corner. It is within this interaction that the disruption generated by the EHR has the potential to be harnessed as a new space for shared engagement. The physical body was once the source of all elements of story, functioning as a lens that concentrated the physician gaze onto the patient. The EHR, however, functions as a prism, scattering that gaze by redistributing the patient’s vital signs, laboratory testing, and imaging results to a virtual space. While this “iPatient” has been bemoaned, often justly so, in physician commentaries (4,9), the EHR, in producing this virtual body, has created an externalized third space upon which the patient, as subject, can actively look, instead of passively being looked upon as an object of the physician gaze.
Indeed, some physician texts reveal a willingness to embrace this approach, with patients and physicians “[working] together on the same side of the screen.”[11] Though recent studies estimate that patients currently spend only about 8-10% of their encounter time gazing at the screen, this has the potential to expand, as screen sharing has been identified broadly as both a core tenet and positive outcome of appropriate EHR use.[11-13] The medical literature contains multiple studies devoted to finding ways to facilitate clinicians and patients sharing screens, and, subsequently, information, via projection of images, portable tablets, or physical reorientation of workspaces to maximize screen sharing.[12-14] Seated side by side, patients have the potential to view the narrative in real-time as it is crafted and typed by their physicians into the chart.
In its previous pen-and-paper format, the medical note remained under lock-and-key in office filing cabinets; subsequent rudimentary electronic data storage systems often were tethered to office-based desktops. The EHR, conversely, has the potential to be accessed from multiple sites and viewed by a variety of users. In an instance of form influencing function, this potential for universal access encoded within the technology of the EHR has effected a change on how the physician note itself is viewed, not just as a record that belongs solely to clinicians and billers within the confines of the healthcare system, but a living document in which patients can have joint ownership outside the borders of the clinical encounter. In 2010, an initiative called OpenNotes demonstrated the potential of the EHR in democratizing access to the medical narrative. In OpenNotes, patients are able and encouraged to view their physicians’ notes from home. One study of this program found that 80% of patients with access to those written narratives felt that they had more control over their care.[15] Traditionally vulnerable and disenfranchised patients, such as racial minorities, the elderly, and non-English speakers, were most likely to report deriving benefit from access to their notes.[16] Many patients also used their access to be able to share their notes with caregivers or family members, demonstrating the portability of the narrative in the EHR era.
Access may, in turn, lead to power. Simply gaining access to these narratives via the EHR appeared to afford patients some indirect influence over the narrative itself; in one study, 20% of physicians participating in the OpenNotes program felt that they subsequently changed the way they wrote about sensitive topics, such as patients’ substance abuse, mental health issues, and obesity.[15] Upwards of 300 institutions across North American currently use OpenNotes, indicating an EHR-engendered paradigm shift in attitudes about who should have access to the physician note.
Moreover, cognizant perhaps of the new limits constricting the physician-storyteller identity within the medical record, physicians are also taking on new identities as co-creators or facilitators of the patient narrative. One physician account notes that EHRs can “foster thoughtful assessment” if clinicians “craft thoughtful differential diagnoses and note unanswered questions together with their patients.”[11] Another encourages clinicians to integrate “patient-generated” reports on status and goals of care into the EHR.[10]Yet another physician describes how she has created custom templates that allow her patients to engage with their care by directly typing their reactions into their record, treating this as a “shared space.”[17]
A nascent initiative called OurNotes takes this a step further, proposing that patients formally co-produce notes with physicians.[18] Ownership of narrative is further placed in patient hands via programs such as the Veterans’ Affairs’ My Life My Story program, developed by two psychiatrists, wherein patients share their stories with volunteers who transcribe this patient-driven narrative and embed it back into the EHR for clinicians to access. Bypassing physicians, patients may also be able to work in concert with technology to create their own histories in the chart. In one example of such electronically-generated histories of present illness (HPIs), patients enter their symptoms into a computer portal, and an algorithm of computerized adaptive testing questionnaires then guides patients through a computerized history-taking process. Information is ordered and prioritized using a combination of patient gestalt and empirical data. Indeed, the only person not contributing any data to this narrative is the physician. A blinded panel of physicians found such computer-generated HPIs to be more complete, useful, succinct, and comprehensible when compared with physician-generated histories.[19] One could argue that such initiatives do not represent any meaningful progress in patient agency, since the narrative is guided by an electronic algorithm; however, the algorithm does in turn adapt to patient responses. Such first steps are representative of the potential for a much more active patient role in guiding, creating, and transcribing their narratives within the medical record, and hold the promise of a new symbiotic relationship between patients and technology.
As physicians, we often perceive that the EHR represents a loss of our own agency, with power being redistributed to administrators, coders, and billers in the fee-for-service model that has shaped the EHR to date. However, the EHR also has the potential to redistribute power to patients, and as such, this loss of power is our gain. As our grasp on the patient narrative loosens, we need not hand over the reins to the larger political, financial, and bureaucratic forces that have driven the adoption of the EHR; we can share that control with our patients. Rather than taking histories from our patients in creating recorded narratives of health and disease, we can engage in co-creating those narratives with our patients as partners, facilitated by an admittedly unlikely mediator.
Kamna Balhara, MD, MA is an assistant professor of emergency medicine and assistant residency program director at the Johns Hopkins University School of Medicine. As a practicing physician and educator, she co-directs the initiative for Health Humanities at Hopkins Emergency Medicine (www.hopkinsem.org/health-humanities) and is currently implementing and evaluating a health humanities curriculum for resident physicians.
Cover Image: UnSplash.com
- Gillum RF. From Papyrus to the Electronic Tablet: A Brief History of the Clinical Medical Record with Lessons for the Digital Age. Am J Med 2013;126:853-7.
- Lambrew J. The White House Blog. https://obamawhitehouse.archives.gov/blog/2013/05/24/more-half-doctors-now-use-electronic-health-records-thanks-administration-policies
- Washington V, DeSalvo K, Mostashari F, et al. The HITECH era and the path forward. New England Journal of Medicine (2017) 377:904-6.
- Verghese A. Culture shock – Patient as Icon, Icon as Patient. N Engl J Med 2008 359;26
- Rosenbaum L. Transitional Chaos or Enduring Harm? The EHR and the Disruption of Medicine. N Engl J Med 2015; 373: 1585-8.
- Hartzband P, Groopman J. Off the record – Avoiding the pitfalls of going electronic. N Engl J Med 2008;358; 1656-8.
- Donato A. The Soul-less Note. Acad Med 2011;86:157.
- Hartzband P, Groopman J. Medical Taylorism. N Engl J Med 2016;374; 106-8.=
- Rosenthal DI, Vergese A. N Engl J Med 2016;375: 1813-5.
- Goroll AH. Emerging from EHR Purgatory – Moving from Process to Outcomes. N Engl J Med 2017;376:2004-6.
- Schiff GD, Bates DW. Can electronic clinical documentation help prevent diagnostic errors? N Engl J Med 2010;362:1066-9.
- Alkureishi MA, Lee WW, Lyons M, et al. Impact of Electronic Medical Record Use on the Patient–Doctor Relationship and Communication: A Systematic Review. J Gen Intern Med 2016;31:548-60.
- Wolfe L, Chisolm MS, Bohsali F. Clinically Excellent Use of the Electronic Health Record: Review. JMIR Hum Factors 2018;5:e10426.
- Yang Y, Asan O. Designing patient- facing health information technologies for the outpatient settings: a literature review. J Innov Health Inform 2016;23:441–9
- Delbanco T, Walker J, Bell SK, et al. Inviting Patients to Read Their Doctors’ Notes: A Quasi-experimental Study and a Look Ahead. Ann Intern Med 2012;157:461-70.
- Walker J, Leveille S, Bell S, et al. OpenNotes After 7 Years: Patient Experiences With Ongoing Access to Their Clinicians’ Outpatient Visit Notes. J Med Internet Res 2019;21:e13876.
- Feldman E. The Day the Computer Tried to Eat My Alligator. JAMA 2010;304:2679.
- Mafi J, Gerard M, Chimowitz H, et al. Patients Contributing to Their Doctors’ Notes: Insights From Expert Interviews. Ann Intern Med 2018;168:302-5.
- Almario CV, Chey W, Kaung A, et al. Computer-Generated Vs. Physician-Documented History of Present Illness (HPI): Results of a Blinded Comparison. Am J Gastroenterol 2015;110:170-9.