Travis Chi Wing Lau //
Very recently, I had a discussion with the brilliant Jillian Weise about naming—in this case, how we name the condition of spinal curvature. In truth, I only recently learned the full name of my specific diagnosis: kyphoscoliosis. This is a compound term in medicine (kyphosis + scoliosis) used to denote both the rounding (which creates what gets colloquially referred to as a “hunchback”), as well as lateral curvature of the spine (which creates the textbook “S-shape”). After having new x-rays done, the report from the imaging center revealed to me the actual name of my condition, which I had always shorthanded as “scoliosis.”
From a narrative medicine standpoint, diagnosis sometimes helps to provide a framework for understanding the disorienting experience of disability. If disability and illness bring about forms of what Arthur Frank has called “narrative wreckage” in which an individual’s narrative of life is disrupted or broken, diagnosis thus offers a form of meaning-making that helps embodied sensation be understood toward new narratives of self. A diagnosis is sometimes the only means by which sick and disabled people are recognized by medicine or even included in communities. Diagnosis can be a rallying point that draws together communities of care and patients and practitioners in solidarity. Here, the act of naming is the act of realization: quite literally making real what can feel like an idiosyncratic, individualized experience.
As Jillian and I both remarked, there are few alternatives to “scoliosis” as a means of identification. Even a cursory search for hashtags and organizations leads repeatedly to “scoliosis” as the primary term. Like many disabled people, I have long had reservations about being defined by medicine—to have my identity reduced to scoliosis, to be the embodiment of scoliosis, to be inseparable from scoliosis. Disability scholars have long pushed back against diagnosis as a technique of medical control, which not only claims to know an individual within the therapeutic or curative parameters of medicine, but also treats an individual as an object of medical intervention or invasion. In this framework of diagnosis, subjectivity is made secondary or only a by-product of the diagnostic act, which is still centered around the power of the medical gaze and the expertise of the physician. Even in the very act of taking patient histories, so often medical providers “sift” and “interpret” the narratives of patients for details indicative of a medical truth but also so often understand these accounts as tangential or even obstacles to diagnostic accuracy. To then identify primarily by this diagnostic name risks reifying this medical objectification as the only means by which disabled subjectivity can come into focus, can matter at all. A name you are given and you shall go by.
My students in my introductory seminar to medical humanities and disability studies asked the perennial question: what is the alternative then? I resonate deeply with queer and crip communities engaging in discursive acts of reclamation: to claim crip is an act of pride and empowerment, cripness is a political identity that exposes the ableist norms of a society never built for us in the first place. But I don’t think it is worth jettisoning “scoliosis” from my identifiers because of how my crip work has come to reinvest in scoliosis as more than “unnatural” curvature or “spinal deformity.” I am indebted to Merri Lisa Johnson who used the term “scoliosis-related disability” to indicate a much larger assemblage of conditions that accompany the curvature of the spine. In my case, these are chronic pain, brain fog, gastrointestinal sensitivity, and anxiety. Here, the naming works against the reductionism of scoliosis as a medical diagnosis. Scoliosis, merely indicative of spinal curvature (which is not always pathological), is not the focus; rather, it is its systemic effects on the body and lived experience. As I have written in my previous essay about being disabled in graduate school, this shift in terminology helped reframe my experience that does not so much perceive the actual degrees of spinal curvature as it does feel fractured into the “episodic, not linear, a matter of intensities, sensations, and situations, not illness and cure” that Johnson so aptly describes of scoliosis. These shifting intensities, sensations, and situations are the stuff of my poetry, the conditions in which I write.
A friend asked me if I felt better now that I “finally knew the actual name of my condition.” For me, the difference is in precision: I can now more aptly describe the physicality of spinal curvature in two planes. But to be honest, knowing my condition’s name changes nothing of the experience of coming into crip consciousness—of learning the contours of my scoliosis-related disability on its own terms that may not fit a medical narrative. It does not change how my body defies the curative impulse to “straighten” up, how it has taught me to inhabit the position of “crip willfulness,” as Johnson puts it. Working my way toward crip consciousness was the project of my chapbook, The Bone Setter, and in many ways, the way I know that “kyphoscoliosis” doesn’t matter is that the poems in that book wouldn’t change even with this difference in diagnostic naming.
Looking again at this printout of a physician’s interpretation of film and bytes of data, I don’t see myself at all. I see only the consequences of what Lennard Davis has described as diagnosis’s “profound ambivalence”: “If you gain knowledge ‘through’ something, is the knowledge gained of the subject or the object? If the object is the means through which you know, then is the knowledge of the subject or the object? What makes the knowledge ‘thorough’ in that case?”[i] The practitioner claims to know me, but I am not present in this account even as I am ironically the matter exposed to the light in the pursuit of bodily truth. The imaging technician, the spine specialist, the chiropractor know through me and because of me. Yet I am to supposed to be indebted to their giving name to my pain, my body’s deformation.
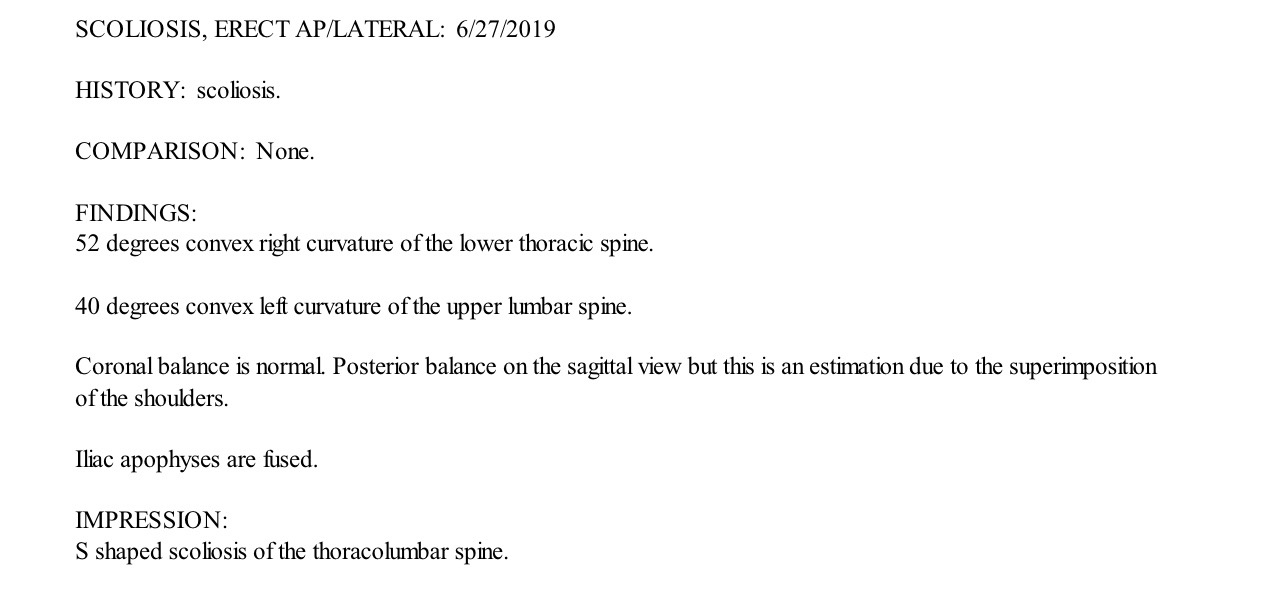
The glaring absence here is what hurts the most: my own name.
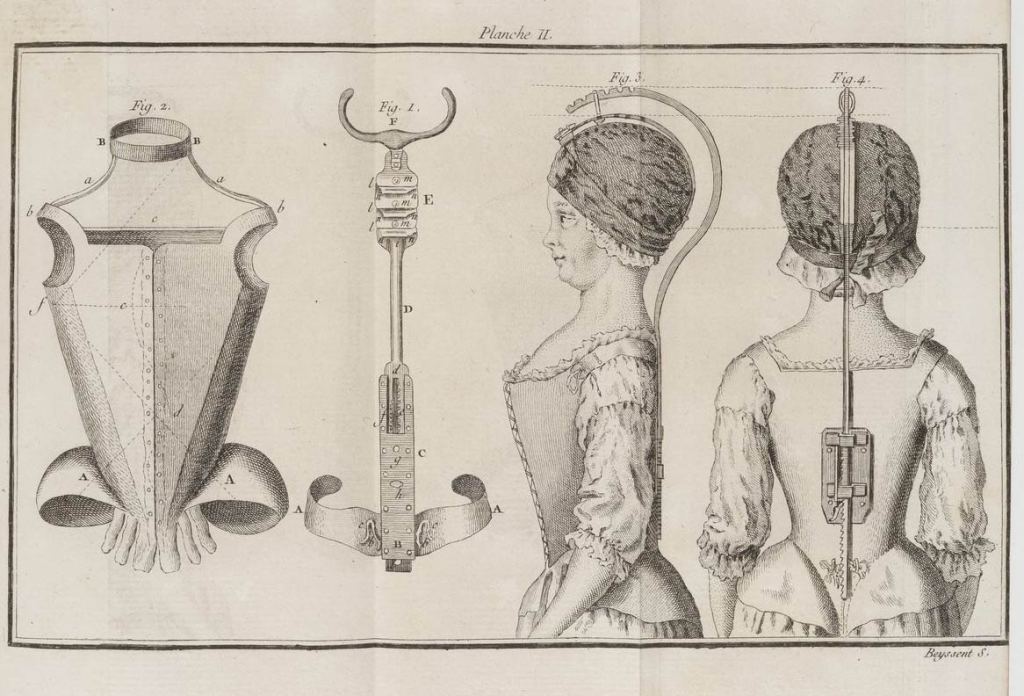
Featured Image: Illustration from ‘Traité du rakitis ou l’art de redresser les enfants contrefaits’ (Paris, 1772), M. Lavaucher de La Feutrie. Source: Wellcome Collection. Public Domain Mark.
[i] The End of Normal: Identity in a Biocultural Era (Ann Arbor: University of Michigan Press, 2013): 85.