
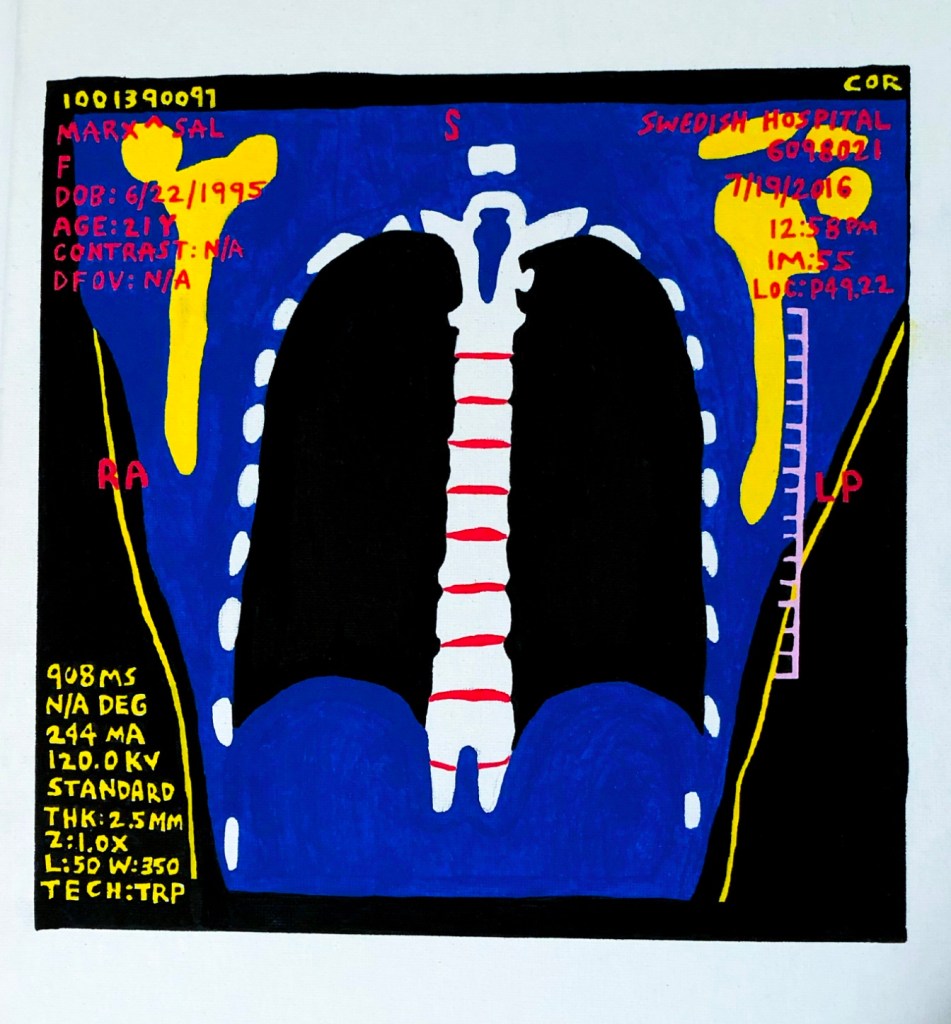
Sal Marx //

Condition on discharge: stable.
Still, I stumbled out of the belly of the hospital, onto pavement, clutching newly prescribed instructions:
1. Avoid physical exertion
2. If you feel worse, go to ER immediately
3. Do NOT use marijuana or other illicit drugs
4. Taper off the drug that treats your Major Depression within 10 days.
It’s almost as if they stigmatize SSRIs more than cannabis. It’s almost as if my body and mind are distinct and one takes priority over the other. It’s almost as if “coordination of care” is a placeholder for “absolving of care.”
I am a barcode, and I was passed along: pulmonology (extensive workup—unremarkable), cardiology (extensive workup—unremarkable), neurology, infectious disease. The list goes on. Symptoms persist, a body needs air. This body beats too fast. Hand my chart to the next MD: a baton in a relay race that has no end in sight, and I am not sure if we are even on the same team.
I had just turned 21. On paper, no longer a child, but I had been tied to machines for too many days: witnessing conversations between doctors and my parents as I lay resigned, tethered to my hospital bed.
They don’t let you feel sunlight, I think, as I stand in the hospital parking lot, trying to drink the sun. I later learn that vitamin D deficiency increases risk for cardiovascular disease.
So why, am I, The Patient in Your Cardiac Hospital, not allowed to feel sunlight?
Brief Reason for Admission: 21-year-old female with a history of ankylosing spondylitis, who is admitted via the emergency department with shortness of breath. Despite little exertion, the patient was tachycardic and hypoxic. Extensive workups remained unremarkable. Upon discharge, few conclusions were made. Our understanding of the complications presented by chronic disease is limited. The questions left unanswered lingered on notepads and “not sures” in the cloud. Note—primary care physician made sense of the situation by labeling the patient as a zebra.
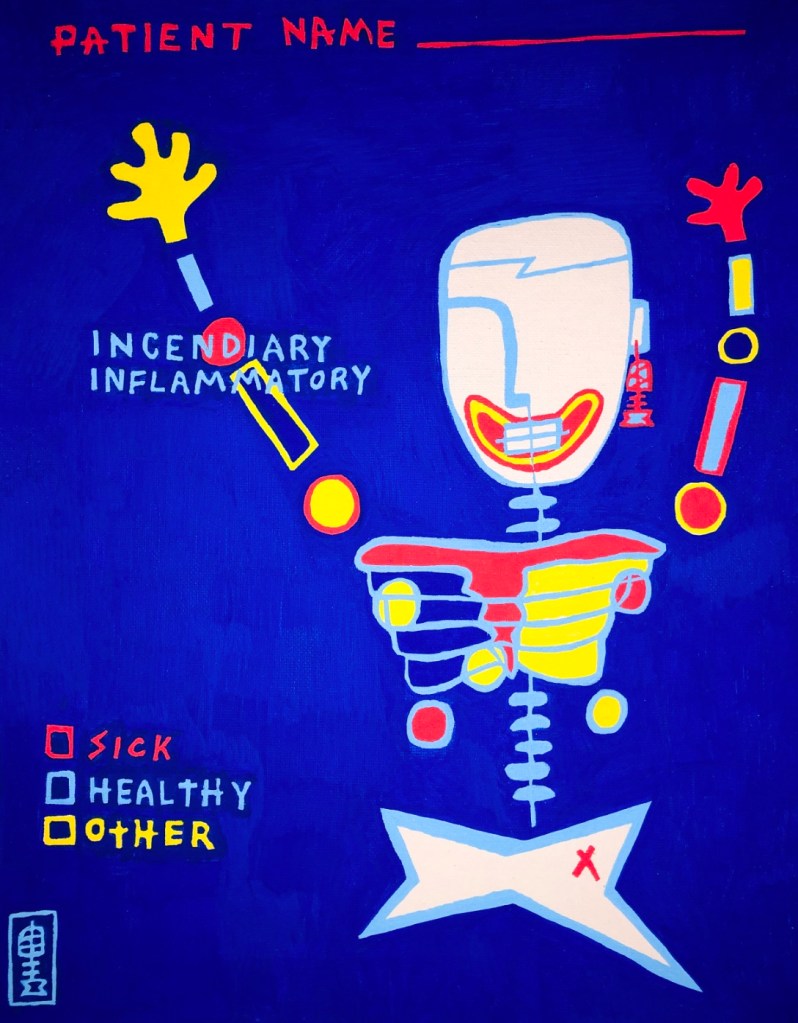
Apparently, in medical school, they teach you to think “logically” in regard to a differential diagnosis. The saying goes: when you hear hoofbeats, think of horses, not zebras. If a patient presents with the flu, you certainly should not entertain a number of other unlikely diagnostic possibilities.
I am a zebra, and I would like to know what determines a diagnostic probability. I am not a zebra, but I am still lying in your hospital bed, for reasons unknown. I am a zebra, and I would like to ask your supervisor: a diagnostic probability by what margin? Whom does your zebra serve to erase?
There is an undeniable coldness that permeates the air in a hospital if you stay too long. I do not mean the stone faces with clipboards in coats but the temperature circulating my sickbed. An insidious chill that takes residency deep in my bones, making home alongside flames, my body inflamed. A hospital gown is designed with one intention: to make the patient’s body accessible during treatment. It is not meant to shield from cold or scare away the sounds that echo through the hallways at night.
I am not a zebra, but I am on high-risk immunosuppressive medication. I am not a child, but this gown is too big and too harsh on my bruised skin as I lay here, asking when my body became too many conflicting bodily systems instead of just one.


Artist bio: Marx is a multimedia artist who works to illuminate patient experiences with chronic disease and disrupt the medical industrial complex. Living with Ankylosing Spondylitis, an invisible, underrepresented disease, they hope to use storytelling to empower patients and promote health justice and equity in the biomedical sphere. Marx is a graduate student in the Narrative Medicine program at Columbia University. salmarx.myportfolio.com


