Tianyuan Huang//
Truth be told, I did not see this coming.
Before the COVID-19 pandemic, I thought I would have been conducting dissertation research in Tokyo for nearly half a year by now; but I am still in New York City awaiting the lifting of travel bans, having already rescheduled flight tickets for the third time. If not for the pandemic, I would perhaps also have shrugged off the phrase “history repeats itself” as an overly simplistic statement that underplays the contingent nature of past events. Yet despite the continuous advancement of medical science since the nineteenth century, the persisting pandemic has succeeded in pushing me through episodes of déjà vu. Sometimes I feel I am being thrown back in time, teleported to Japan—the geographic focus of my research and where I desperately need to be—amid the 1918 influenza pandemic.
“Do not go out even if you only coughed once!”
“Do not forget about the mask!”
“Get your vaccine shot as soon as possible!” (Tōkyō Asahi shinbun 1920)
Circulated in January 1920, these were but some of the many resounding warnings that Japanese newspapers deployed to raise public awareness as the emergent East Asian empire was thrusted into the third calendar year of a deadly pandemic. By then, public policy measures had taken place at multiple levels and areas of jurisdiction. The Metropolitan Police Department had urged Tokyo residents to keep indoor areas clean, avoid crowds, and quarantine the infected in isolation (Tōkyō Asahi shinbun 1918a). The Ministry of Education had advised on the close of schools to prevent the spread of pathogens (Tōkyō Asahi shinbun 1918b). The Ministry of Home Affairs, upon recognizing the pandemic’s transnational impact, collected overseas intelligence through the Imperial Navy and the Ministry of Foreign Affairs to distribute to local administrations (Tōkyō Asahi shinbun 1918c).
In comparison, our responses to COVID-19—be they social distancing, mask-wearing, or vaccination—appeared astoundingly reminiscent of a road the imperial Japanese government had once taken. Not to mention, the beginning of 2022 also marked the third calendar year of our own experience of living with disruptive uncertainty. This eerie coincidence begs not only the question of what additional paths could have been explored, or explored more seriously, over a century ago to end the plight sooner, but also the question of what we could be doing above and beyond mask-wearing and vaccination. After all, the coronavirus has been vigorously evolving, with the Omicron variant being the most recent evidence. Shouldn’t our approach to healthcare do, too, in recognition of the need for adaptation?
As far as Japanese society is concerned, responses to the 1918 pandemic exhibited at least one bias blind spot from which we can perhaps still learn a lesson. Namely, the potential of indigenous and traditional medicine in providing healthcare alongside biomedicine was frustratingly under-explored and insufficiently, if at all, documented in official reports (Rice and Palmer 1993).
To be sure, the initiative to mobilize indigenous and traditional medical knowledge to help address the 1918 pandemic was not absent within the Japanese medical community. Published in the 25 September 1920 issue of Ikai jihō (Medical Times), an essay asked the public not to forget “imperial Chinese medical doctors” (kōkan-i)—physicians who practiced Chinese-style herbal medicine (kanpō) as opposed to biomedicine—in combating the influenza (“Ryūkan to kōkan igaku” 1920).
In Nara prefecture, according to the essay, one senior kanpō physician had succeeded in keeping the infection rate low in local communities by mass-distributing traditional formulas of pharmaceuticals as a preventive measure. Nonetheless, masks and vaccines dominated the official discourse surrounding the effective solutions to a public health crisis. Unsurprisingly, the essay attributed the lack of recognition of traditional medicine’s potential merits to the then common mindset among Japanese health professionals where “medicine is confined to Western medicine,” “Western medicine is almighty,” and “science is omnipotent” (“Ryūkan to kōkan igaku” 1920).
“Medicine is confined to Western medicine”
“Western medicine is almighty”
“Science is omnipotent”
Although the essay’s bitterness towards Western medicine and science seems to border dangerously on the sentiments of some of the COVID-19 anti-vaxxers of our day, it was not an entirely unwarranted reaction in its own historical context. En route to realizing the goals of “enriching the country, strengthening the military” (fukoku kyōhei), the Meiji state of Japan (1868–1912) eagerly sought after what the historian Ruth Rogaski (2004) describes as a “hygienic modernity.” In certain cases, being “modern” meant emulating the West. The official medical licensing exam, for instance, was then designed to test exclusively participants’ knowledge of chemistry, physics, and other subjects of biomedicine. Inevitably, the state-sponsored institutionalization of biomedicine in the emerging landscape of public health came at the cost of kanpō and other forms of alternative medical knowledge, whose history, epistemology, and clinical efficacy medical science could not yet fathom or measure. To be sure, political efforts were made to revise the medical licensing exam so as to allow participants to take the test in subjects of either Western or kanpō medicine during the last decade of the nineteenth century. Yet at the time, such attempts to preserve traditional knowledge failed to come into fruition. To some policy makers, medicine had come to function mechanically as a “weapon against disease” and, in this analogy, traditional East Asian medicine represented no more than the outdated “bows and arrows,” bound to give place to the “guns” that Western medicine embodied and responsible for its own and perceived-to-be inevitable demise as outdated folk superstitions (Teikoku gikai 1895, 7).
To some policy makers, medicine had come to function mechanically as a “weapon against disease”
Today, some have come to see the relations among different systems of medicine in a new light, not as one of zero-sum rivalry but one where they may complement, inform, and thrive with one another. The most recent and eleventh revision of the International Classification of Diseases, for example, has unprecedentedly included a standalone chapter on traditional medicine (WHO 2018). Since the early stage of the COVID-19 pandemic and well before vaccines or antiviral agents became available, some researchers have called for more clinical studies on the potential efficacy of traditional Iranian, Indian, and Chinese herbal medicine in preventing and/or treating COVID-19 (Mirzaie et al. 2020). However, whether the idea of intentionally combining the forces of different systems of medical knowledge during a pandemic would elude us again—or be ridiculed as a frivolous thought by default, given only insufficient attention, or be adopted only blindly by policy makers without robust clinical data to back it up—remains a matter subject to future evaluation.
At this point, it has perhaps also become fairly difficult to deny that the scope of the health crisis we currently face exceeds far beyond what infection case numbers alone can describe. The “pandemic” includes that of a mental health catastrophe, too, along with a brutal exposure of existent socioeconomic, racial, and gendered injustices that not only prevent individuals from receiving quality healthcare but also jeopardize their opportunities of education and employment. Medical science can and is helping tackle the coronavirus; there is little double about that. But what about the trauma from grief and isolation, the intangible fear for our collective future, and the fatigue of being constantly deprived of control of our lives for nearly two “stolen” years? How are we going to heal if the wounds are sometimes beyond what randomized controlled trials alone can measure?
It is not my position to pass judgement on historical actors whose motivations and decisions were contextualized by their own time and, in turn, differ from ours. Yet I wonder if the propensity of Japanese observers over a century ago to view medicine as a weapon and disease an enemy, as well as the mentality to trivialize medical knowledges that differ from biomedicine in their ways of knowing and healing so automatically and readily had missed a crucial point about healthcare—a humanistic standpoint. As Rita Charon reminds us in her examination of the power of narrative medicine, “[t]he truth of disease is pain, isolation, and hopelessness…” (Charon 2006, 19). Our ordeal and resilience during the COVID-19 pandemic, dare I say, are also part of this truth—a truth at times too emotional, subjective, and unevenly lived to be a subject for the scrutinization of medical science alone. Moving forward, I hope our responses to COVID-19 would allow future historians to describe a nonlinear, but nonetheless robust path that would eventually lead to a rethinking of the relations between biomedicine and indigenous/traditional medicines, as well as the nature of medicine, disease, and healing in general.
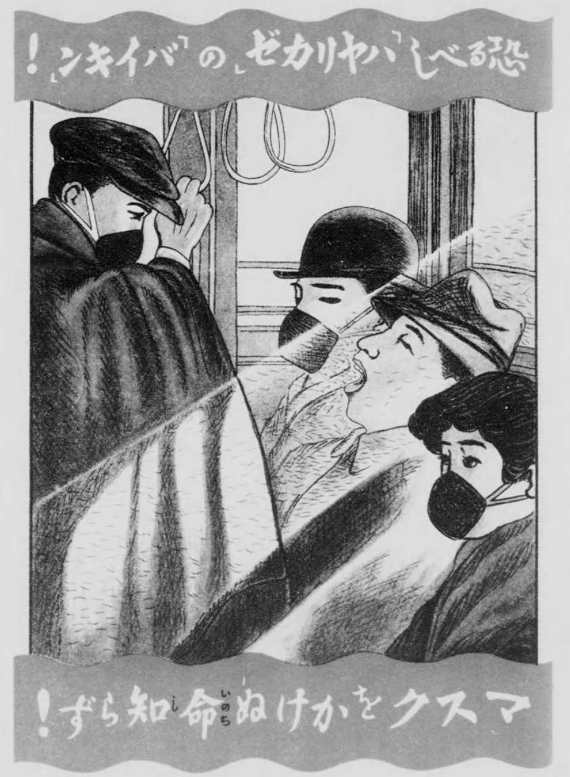
Cover Image
Naimushō eiseikyoku [Hygiene Bureau, Ministry of Home Affairs], Ryūkōsei kanbō [Influenza] (Tokyo: Naimushō eiseikyoku, 1922), 132–133, https://dl.ndl.go.jp/info:ndljp/pid/985202/94. Accessed January 7, 2022 via the National Diet Library Digital Collections. The caption reads “Terrifying ‘germs’ of the ‘influenza!’ Without wearing a mask your life will be at risk!”
Reference List
Charon, Rita. 2006. Narrative Medicine: Honoring the Stories of Illness. New York: Oxford University Press.
Mirzaie, Amir, Mehrdad Halaji, Farhad Safarpoor Dehkordi, Reza Ranjbar, and Hassan Noorbazargan. 2020. “A Narrative Literature Review on Traditional Medicine Options for Treatment of Corona Virus Disease 2019 (COVID-19).” Complementary Therapies in Clinical Practice 40 (August): 101214. https://doi.org/10.1016/j.ctcp.2020.101214.
Rice, Geoffrey W., and Edwina Palmer. 1993. “Pandemic Influenza in Japan, 1918–19: Mortality Patterns and Official Responses.” Journal of Japanese Studies 19 (2): 389–420. https://doi.org/10.2307/132645.
Rogaski, Ruth. 2004. Hygienic Modernity: Meanings of Health and Disease in Treaty-Port China. Berkeley: University of California Press.
“Ryūkan to kōkan igaku.” 1920. Ikai jihō, no. 1370 (September): 9.
Teikoku gikai. 1895. “Dai 8 kai teikoku gikai shūgiin giji sokkiroku, no. 25.” Database System for the Minutes of the Imperial Diet. https://teikokugikai-i.ndl.go.jp/minutes/api/emp/v1/detailPDF/img/000813242X02518950206.
Tōkyō Asahi shinbun. 1918a. “Sekaiteki ryūkō no Supein kaze,” October 25, 1918. Kikuzō II bijuaru for libraries.
———. 1918b. “Monbu bōeki tsūchō,” October 27, 1918. Kikuzō II bijuaru for libraries.
———. 1918c. “Keiji sōkan no kokuyu,” October 27, 1918. Kikuzō II bijuaru for libraries.
———. 1920. “Kono osoroshiki shibōritsu wo miyo, ryūkan no kyōfu jidai shūrai su,” January 11, 1920. Kikuzō II bijuaru for libraries.
WHO (World Health Organization). 2018. “WHO Releases New International Classification of Diseases (ICD 11).” World Health Organization. June 18, 2018. https://www.who.int/news/item/18-06-2018-who-releases-new-international-classification-of-diseases-(icd-11).


